Only 2% to 3% of patients with this malignancy are never smokers4,5; thus, as tobacco exposure causes SCLC in over 97% of cases, its incidence rates mirror smoking patterns. Peak cigarette consumption occurred in the 1960s, but declined following the Surgeon General’s report linking smoking to cancer and the subsequent ban on tobacco advertising on television.6 The percentage of men who smoke decreased from 50% in 1965 to 21.6% in 2011, which is a much greater proportional reduction than in women, who went from a rate of 32% to 16.5% during the same time period.6,7 Correspondingly, the incidence of SCLC in men peaked in 1984 and since has been trending steadily down, whereas in women, the incidence peaked later and only has declined slightly.8 The gender gap has narrowed such that currently about half of the patients diagnosed with SCLC are women (see Fig. 42.1).
Anatomy and Pathology
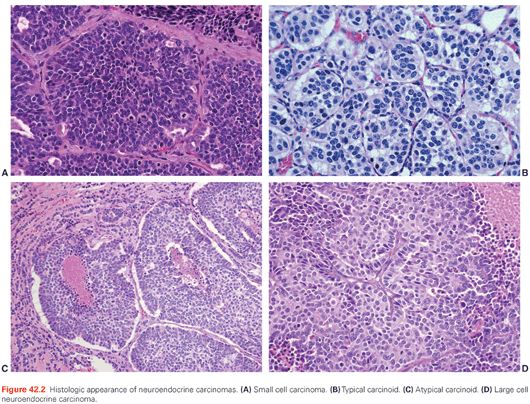
Neuroendocrine tumors of the lung encompass a spectrum of tumors, including low-grade typical carcinoid, intermediate-grade atypical carcinoid, high-grade large cell neuroendocrine carcinoma (LCNEC), and SCLC.9 Because of their shared neuroendocrine properties, these tumors have common morphologic, ultrastructural, immunohistochemical, and molecular features. Despite this, there are also important differences in clinical, epidemiologic, histologic, and molecular characteristics.
SCLC is readily diagnosed on small specimens such as bronchoscopic biopsies, fine-needle aspirates, core biopsies, and cytology. The diagnosis of SCLC is based primarily on light microscopy (Fig. 42.2A): dense sheets of small cells with scant cytoplasm, finely granular nuclear chromatin, inconspicuous or absent nucleoli, and frequent mitoses. Necrosis is common and frequently shows large areas. The tumor cells usually measure less than the diameter of three small resting lymphocytes. They are round to be fusiform in shape and have scant cytoplasm. The nuclear chromatin is finely granular and nucleoli are inconspicuous or absent.9–11 The mitotic rate is characteristically high, averaging 60 to 80 per 2 mm2. Crush artifact is a frequent finding in small transbronchial or mediastinal biopsy specimens and can make pathologic interpretation difficult. The tumor cells of SCLC also have a tendency to show a streaming artifact. This can also occur with non–small-cell lung cancer (NSCLC), lymphoma, and chronic inflammation. In surgically resected specimens where the tumor cells achieve better fixation, the cells of SCLC appear larger than in small biopsies.10,12 When a component of NSCLC, including adenocarcinoma, squamous cell carcinoma, large cell carcinoma, spindle cell carcinoma, and giant cell carcinoma, is present, the term combined SCLC is used with mention of the specific histology of the non–small-cell component.9,10 In resected specimens, combined SCLC may occur in up to 28% of cases.10 To diagnose combined SCLC and large cell carcinoma, the large cell carcinoma component must comprise at least 10% of the overall tumor.9,10
The following immunohistochemical stains are helpful in difficult cases. A pancytokeratin antibody such as AE1/AE3 is useful to confirm if the tumor is a carcinoma. Neuroendocrine differentiation can be demonstrated using a panel of markers such as CD56, chromogranin, and synaptophysin. However, up to 10% of SCLCs may be negative for all neuroendocrine markers.13 A high proliferation rate of 80% to 100% should be seen with Ki-67. Thyroid transcription factor-1 (TTF-1) is positive in 70% to 80% of small cell carcinomas.14–16 Notably, TTF-1 can be positive in extrapulmonary small cell carcinomas, so it is not useful in determining the primary site of small cell carcinomas.17
Genetics
SCLC has been characterized by frequent inactivating mutations in the critical tumor suppressor genes TP53 (75% to 90%)18 and RB1 (60% to 90%).19,20 A mouse model with conditional inactivation of these two tumor suppressors in the lung generates lung tumors histologically and biologically similar to human SCLC.21
Recent reports including exome, transcriptome, and limited whole genome sequencing have provided insights into the fuller landscape of genetic alterations in SCLC.22,23 In addition to confirming TP53 and RB1 inactivation, these studies define other alterations of interest in SCLC, with potential therapeutic implications. One consistent finding from both reports was an exceptionally high degree of genomic alteration in this tumor type, including mutations, insertions, deletions, large scale copy number alterations, and gross inter- and intrachromosomal rearrangements. MYC family member alterations, including gene amplification of MYC, MYCN, and MYCL1, as well as a recurrent gene fusion involving MYCL1, are frequent in SCLC and may represent important drivers of SCLC oncogenesis. The tumor suppressor phosphatase and tensin homolog (PTEN) appears to be inactivated in approximately 10% of SCLC, and mutations of other factors in the same signaling pathway were also identified. Other alterations implicated as potential drivers in subsets of SCLC include amplification of the tyrosine kinase FGFR1 (in 6% of cases) and of the developmental regulator and transcription factor SOX2 (in up to 27% of cases). The therapeutic implications of the large majority of the genetic alterations documented to date in SCLC have not been defined.
Several reports have described the rare phenomenon of transformation to SCLC as a mechanism of acquired resistance to epidermal growth factor receptor (EGFR) tyrosine-kinase inhibitors (TKI) in patients initially treated for EGFR-mutant lung adenocarcinomas.4 Of those cases with acquired resistance to EGFR TKIs, 3% to 14% will undergo SCLC transformation. Importantly, pure SCLC lack EGFR mutations and ALK rearrangements, even in those patients with this malignancy who are never smokers.4,24 However, in the rare cases of SCLC transformation as a mechanism of acquired resistance to EGFR TKIs, there is persistence of the original EGFR mutation in the tumors confirmed on biopsy. In all cases where SCLC has been documented as a mechanism of acquired resistance to EGFR TKIs, the original tumor was a pure adenocarcinoma prior to EGFR TKI treatment, and the transformation was validated by histologic examination and confirmed by expression of neuroendocrine markers.
Screening
Screening computed tomography (CT) scans detect NSCLCs at an earlier stage compared to chest x-ray (CXR), or no screening, and can decrease lung cancer–specific mortality in heavy smokers.25 However, the natural history of SCLC is characterized by rapid tumor growth and early metastatic spread. As such, the diagnosis of SCLC in an asymptomatic patient is rare. The National Lung Screening Trial (NLST) enrolled 53,454 Americans age 55 to 74 years with a history of at least 30 pack-years of cigarette smoking, and randomly assigned them to undergo three annual screenings with either low-dose CT scans (LDCT) or standard CXR. LDCT screening identified a preponderance of adenocarcinomas, including many with bronchioloalveolar subtype. SCLCs were not detected at early stages by either LDCT or CXR in the NLST. Although the study demonstrated a reduction in lung-cancer specific mortality compared to CXR, the similar rates and patterns of detection of SCLC make it unlikely that LDCT screening will reduce mortality specific to SCLC. Therefore, screening for SCLC by any method is not recommended.25
Diagnosis
Presenting symptoms in patients with SCLC can be constitutional, pulmonary, the result of extrathoracic spread, or due to paraneoplastic disorders.26,27 In one series in which patient-reported symptoms were recorded using the Lung Cancer Symptom Scale, fatigue was the most common, symptom with decreased physical activity, cough, dyspnea, decreased appetite, weight loss, and pain occurring sometime in the course of the illness in the majority of patients.27 Hemoptysis was noted in 14% in the same series.27 The primary tumor often presents as a large central mass invading or compressing the mediastinum. Superior vena cava obstruction is present at diagnosis in 10% of patients with SCLC (Fig. 42.3),28 and in these cases, the symptoms are often worsened by associated thrombosis in the compromised blood vessel. Chest imaging typically shows hilar and mediastinal adenopathy. Rarely, SCLC presents as a solitary pulmonary nodule.29,30 No more than 2% of SCLC present as a superior sulcus tumor.31
Most patients with SCLC have metastases at diagnosis. Bone involvement is usually characterized by osteolytic lesions, often in the absence of bone pain, or elevations in the serum alkaline phosphatase.32 Osteoblastic bone metastases do occur in some patients. Hepatic and adrenal lesions are typically asymptomatic. Brain metastases can be detected in at least 18% of patients at diagnosis,33 which are often asymptomatic.
Paraneoplastic syndromes are common in SCLC and differ from those observed with NSCLC. SCLC accounts for approximately 75% of the tumors associated with the syndrome of inappropriate antidiuretic hormone (SIADH). Although serum concentrations of antidiuretic hormone are elevated in the majority of those with SCLC, only approximately 10% of patients fulfill the criteria of SIADH, and symptoms are present in no more than 5%. In some cases, ectopic production of atrial natriuretic factor contributes to the disorder in sodium homeostasis. The primary treatment for hyponatremia in SCLC patients is chemotherapy aimed at treating the disease. Additional management strategies include fluid restriction in mild cases or intravenous hypertonic saline in severe, symptomatic cases. Older pharmacologic interventions that have been used in SIADH, include demeclocycline and lithium, both of which induce nephrogenic diabetes insipidus.34 More recently, tolvaptan, an oral vasopressin V2-receptor antagonist, has been shown to significantly improve serum sodium in patients with SIADH over a 4- and 30-day period.35 Tolvaptan therapy should be initiated while patients are in the hospital to allow monitoring of the therapeutic response. Increased serum levels of adrenocorticotropic hormone can be detected in up to 50% of patients with lung cancer, but Cushing syndrome develops in only 5% of patients with SCLC. Low serum sodium is an adverse prognostic factor,36 and patients with Cushing syndrome have a very limited survival.37 The primary treatment of Cushing syndrome in SCLC patients is chemotherapy, although agents such as ketoconazole and mitotane have been used.38 Hypercalcemia is rare in SCLC.
Paraneoplastic neurologic disorders seen in patients with SCLC include sensory, sensorimotor, and autoimmune neuropathies and encephalomyelitis.39 These syndromes are thought to occur through autoimmune mechanisms, and antinuclear antibodies that bind to SCLC and to neuronal tissues have been identified. Symptoms may precede the diagnosis by many months and are often the presenting complaint. They may also be the initial sign of relapse from remission. An aggressive search may be required to discover small tumor nodules causing profound neurologic syndromes. Subacute peripheral sensory neuropathy associated with the anti-Hu antibody may be the most frequent paraneoplastic neurologic disorder seen in those with SCLC. Less common is the Lambert-Eaton syndrome, characterized by proximal muscle weakness that improves with continued use, hyporeflexia, and dysautonomia. Classic electromyographic findings confirm the diagnosis. The cause is related to autoantibody impairment of voltage-gated calcium channels. Rarer neurologic disorders seen in patients with SCLC include cerebellar degeneration or retinopathy. Two studies conflicted when evaluating whether the presence of paraneoplastic antibodies have prognostic implications40,41; the utilization of different techniques to measure antibody levels may account for the discrepant results.42
In contrast to the endocrine syndromes, for which successful treatment of the tumor effectively controls the symptoms, the occurrence and severity of the neurologic symptoms is unrelated to tumor bulk and usually does not resolve with antineoplastic therapy. Various therapies such as plasma exchange and immunosuppressive therapy with agents such as corticosteroids, cyclophosphamide, and tacrolimus have been tried, but generally offer little benefit. In patients with Lambert-Eaton syndrome, two randomized placebo-controlled trials of 3,4 diaminopyridine, which blocks potassium channel efflux from nerve terminals, demonstrated that treatment with this agent increases compound muscle action potentials and significantly improves muscle strength.43 In a randomized trial with a crossover design, intravenous immunoglobulin also improved limb strength as measured by myometry over placebo in 10 patients with Lambert-Eaton syndrome.43 However, the benefit was short lived and began to dissipate after just 8 weeks.
Staging
A simple two-stage system, introduced by the Veterans’ Administration Lung Study Group (VALSG), has historically been utilized instead of the tumor, node, metastasis (TNM) system employed for most other cancer types.44 In the VALSG system, limited stage is defined as disease confined to one hemithorax that can be “encompassed” in a “tolerable” radiation field. These patients currently are treated with a combined modality approach. All other patients are considered to have extensive-stage disease. At presentation, approximately two-thirds of patients with SCLC have extensive disease and one-third have limited-stage disease.1
In the VALSG staging system, the appropriate classification of ipsilateral pleural effusion, supraclavicular lymphadenopathy (ipsilateral or contralateral), or contralateral mediastinal lymphadenopathy as either limited or extensive stage remains controversial. Some large series have not found a survival difference between patients with an isolated ipsilateral pleural effusion and other patients with limited SCLC.45 However, analyses of two large cooperative group databases, which included over 4,000 patients, showed that the survival of individuals with an isolated effusion was similar to that of patients with extensive disease.46,47 In clinical practice, it is assumed that an effusion is malignant unless three criteria are met: the fluid is transudative, nonhemorrhagic, and cytologically negative on repeated examinations. Patients with a malignant effusion are appropriate to exclude from a combined modality treatment because hemithoracic radiotherapy to encompass the entirety of the pleura is impractical.
The presence of supraclavicular lymphadenopathy commonly is associated with extensive disease but, when encountered in patients with otherwise limited disease (5% of cases), carries a trend toward poorer survival.47 Contralateral mediastinal involvement also is usually classified as limited-stage disease. However, two studies that evaluated twice-a-day radiation regimens excluded patients with contralateral hilar disease to reduce the normal lung volume irradiated and the risk for toxicity.48,49
For patients who appear to have limited-stage SCLC, some additional tests may be appropriate to confirm this assessment. Unilateral iliac crest bone marrow aspiration and biopsy are still a routine part of staging for many oncologists and should be performed in limited-stage patients with elevations of serum lactate dehydrogenase (LDH)50,51 and evidence of myelophthisis (nucleated red blood cells, leukopenia, or thrombocytopenia) on the peripheral blood smear. If there is evidence of a pleural effusion, a thoracentesis or thoracoscopy may help confirm that the effusion is nonbloody, transudative, and cytologically negative. Effusions too small to permit image-guided sampling should not be considered in staging.52 Osseous abnormalities seen on positron-emission tomography (PET) or bone scan require confirmation with magnetic resonance imaging (MRI), CT scan, or biopsy if they represent the only disease site that makes a patient extensive stage.
For the American Joint Committee on Cancer (AJCC) seventh edition, the use of a TNM staging system for SCLC has been revisited. To establish the accuracy of outcomes based on stage, cases of completely resected SCLC were staged using the same definitions as used for NSCLC.53 The use of pathologic stage was necessary to accurately stage the patients used for this analysis. More favorable outcomes of patients have been reported in patients previously classified as very limited disease (i.e., no evidence of mediastinal metastases by CT or mediastinoscopy) treated with chemotherapy and radiation, as compared with other patients with limited-stage disease.54,55,56 The use of the TNM system is best applied for cases of early stage disease and may have less relevance for the majority of patients presenting with metastatic disease.
Clinical and Serologic Predictive and Prognostic Factors
Multivariable analyses suggest that performance status is a strong and reproducible predictive and prognostic factor.47,57,58 Poorer performance status can additionally identify individuals at higher risk for treatment-related complications. Several other clinical parameters have been proposed. Female gender has been associated with improved response and survival in patients with SCLC.47,57,58 Older age (variably defined) has not been identified as an adverse prognostic factor in patients with SCLC in most59–62 but not all36,46,47 series. Older age has been associated with decreased performance status and more comorbid illnesses and often results in compromised chemotherapy dose intensity,63,64 which may partially explain its prognostic implications. Certain metastatic sites, such as the liver,65–67 the brain,66,68 bone marrow,67 and bone,68 as well as the total number of metastatic sites involved,47 have been found to be of prognostic significance for patients with extensive-stage disease. Paraneoplastic Cushing syndrome has been correlated with a poor response to therapy and short survival.37 Continued use of tobacco during combined modality therapy was identified as an adverse prognostic factor in a group of 186 patients with limited disease.69 Elevation of serum LDH is found in 33% to 57% of all patients with SCLC and up to 85% of patients with extensive-stage disease and is a strong prognostic and predictive factor.46,57,65,66,68,70–72 Serum LDH elevation is associated with the presence of bone marrow involvement.50 Although many other serum markers have been proposed to have prognostic significance, including neuron-specific enolase,61,66 chromogranin, and precursors of gastrin-releasing peptide,73,74 none have been strong and reliable enough to warrant general use. Carcinoembryonic antigen (CEA) has been found to predict outcome in SCLC in multiple series.57,75,76
Management by Stage
General Recommendations for Initial Management
Once the pathologic diagnosis of SCLC is confirmed, a complete history and physical examination is the next step. Special attention should be paid to the cigarette smoking history. If a patient is a current smoker, he or she should be advised to quit immediately in the strongest terms and offered the most aggressive smoking cessation intervention available.69 If the patient is a never smoker, the pathologic diagnosis of SCLC should be reviewed as only 2% to 3% of never smokers develop SCLC.4,5 The National Comprehensive Cancer Network (NCCN) has compiled consensus guidelines for the initial evaluation of individuals with SCLC.52 A complete blood cell count (CBC) with platelet count, electrolytes, calcium, creatinine, blood urea nitrogen (BUN), liver function tests, and LDH are recommended. All patients should undergo a contrast-enhanced CT scan of the chest, a gadolinium-enhanced MRI of the head, and whole-body PET or a bone scan. A PET scan can identify sites of metastases undetected by other modalities77–79 and can replace the bone scan.80
All fit patients (Karnofsky performance status greater than 60% or Eastern Cooperative Oncology Group [ECOG] performance status 0, 1, or 2) should initially receive combination chemotherapy with etoposide plus either cisplatin or carboplatin for four to six cycles (Fig. 42.4).52 Supportive data, specifics of chemotherapy regimens, duration of therapy, and alternatives for patients with contraindications or special needs are discussed in the sections that follow. Patients with limited-stage disease should receive the chemotherapy concurrently with twice-daily thoracic irradiation beginning with the first, second, or third cycle.49,81,82 Patients who achieve a response to chemotherapy should receive prophylactic whole-brain radiotherapy at the conclusion of chemotherapy or chemoradiotherapy.83 There is no routine recommendation for the treatment of patients who have a Karnofsky performance status of 50% or less or ECOG performance status 3 or 4. Because the toxicity of all treatment worsens and effectiveness lessens in patients with a low performance status, clinicians must carefully evaluate the agent(s) used and the appropriateness and goals of therapy individually. For many patients in this low performance status group, supportive care only and referral to hospice are the best options.
Chemotherapy
Evolution of Chemotherapy Regimens. The sensitivity of SCLC to chemotherapy agents was recognized about 50 years ago, and the primary role of systemic treatment in SCLC was established early on. Alkylating agents, anthracyclines, vinca alkaloids, and antifolates all showed single-agent efficacy. In the 1980s, the epipodophyllotoxin, etoposide, and the platinum analogs, cisplatin and carboplatin, were introduced, and their activity ranged from 40% to 60% in previously untreated patients.84 Since then, numerous other chemotherapeutic agents have demonstrated activity in SCLC, but aside from the camptothecins, the drugs identified in the 1970s and 1980s remain the backbone of therapy. Ultimately, randomized trials of combinations demonstrated superior activity to single agents.85,86
Livingston et al.87 developed the cyclophosphamide, doxorubicin, vincristine (CAV) combination, and reported on 358 patients who received this combination followed sequentially by thoracic and brain irradiation. For patients with extensive disease, the complete response rate was 14%, the overall response rate was 57%, and the median survival was 26 weeks. For patients with limited disease, the rates were 41%, 75%, and 52 weeks, respectively. With these data, CAV became the standard chemotherapy regimen.
With the identification of etoposide as perhaps the most active agent, several modifications of the CAV regimen that included etoposide were tested. A randomized trial showed greater response duration and survival with cyclophosphamide, doxorubicin, and etoposide (CAE) compared with CAV.88 Hong et al.89 compared intensive cyclophosphamide and vincristine (CV) (with the dose of cyclophosphamide increased from 1,000 to 2,000 mg/m2) to CAV and to cyclophosphamide, etoposide, and vincristine (CEV) and reported that patients treated with CV had a shorter survival and experienced more myelosuppression than those treated on the other two arms. Five randomized trials have evaluated the addition of etoposide (CAVE) to the CAV regimen.90–94 In the three studies in which the doses of CAV were equivalent in each arm,90–92 a better response rate was evident in the arm that contained etoposide, in at least some patient subsets, with increased hematologic toxicity, although a nonstatistical improvement in survival was seen in only one study.90 Two studies intensified components of this regimen in the CAV arm compared to the CAVE arm,93 leading to equivalent myelotoxicity, response rates, and survival.
The etoposide/cisplatin (EP) regimen was tested in SCLC cases because this combination produced synergistic activity in preclinical systems. In addition, both agents could be given at full doses because of less myelosuppression with cisplatin. The first report by Sierocki et al.95 at Memorial Sloan-Kettering Cancer Center in 1979 demonstrated the activity of this combination in SCLC. Subsequent studies by Evans et al.96,97 reported response rates of 55% in patients previously treated with CAV and 86% in newly diagnosed patients. Einhorn et al.98 reported that two cycles of consolidation with EP, when added to the treatment of patients with limited disease who were responding to six cycles of CAV, produced longer survival than with CAV only. Three randomized trials have compared EP to cyclophosphamide, vincristine, and an anthracycline.99–101 Less myelosuppression occurred with EP, and, if given with radiation, patients experienced less esophagitis and interstitial pneumonitis. Furthermore, the largest trial showed that EP produced a better median (15 months versus 10 months) and 5-year (10% versus 3%) survival for patients with limited disease.101 Retrospective analyses and meta-analyses also support the superiority of cisplatin- or carboplatin-containing chemotherapy for SCLC.102–104 As a result, EP is now the standard first-line chemotherapy regimen for SCLC (Table 42.1).
Carboplatin has been substituted for cisplatin in SCLC chemotherapy regimens in an effort to decrease nonhematologic toxicities. Randomized trials comparing cisplatin and carboplatin suggest that they may have similar efficacy. The Hellenic Cooperative Oncology Group randomized 147 patients with either limited or extensive disease to receive etoposide 100 mg/m2 days 1 to 3, and cisplatin 100 mg/m2 or carboplatin 300 mg/m2.105 Concurrent radiation also was administered to responding patients starting with the third cycle. Response and survival were similar in the two arms. Nausea, vomiting, nephrotoxicity, and neurotoxicity were significantly lower in the patients who received carboplatin, as was grade 4 leukopenia. However, the sample size of this study is inadequate to confirm equivalent efficacy. A meta-analysis that evaluated individual subject data from four randomized trials with a total of 663 patients found that median overall survival (OS), median progression-free survival (PFS), and response rates were similar in the cisplatin and carboplatin arms. Although hematologic toxicities were higher in those patients that receive carboplatin, nonhematologic toxicities were increased in those that receive cisplatin.106 Based on these data, etoposide and carboplatin can be considered an appropriate first-line regimen, particularly in patients who cannot tolerate cisplatin.
More recently, platinum combinations with topotecan and irinotecan have emerged as potential regimens for initial therapy. Irinotecan was shown to have single-agent efficacy in Japanese studies.107 The Japan Clinical Oncology Group compared cisplatin and irinotecan to EP as initial treatment in extensive disease.108 The study was terminated after 154 of the planned 230 patients were enrolled because median (12.8 months versus 9.4 months) and 2-year (19.5% versus 5.2%) survival were significantly better in the group treated with cisplatin and irinotecan. Significant diarrhea occurred only in the irinotecan group, and myelosuppression was the most common toxicity in both groups and more frequent with EP. Two confirmatory studies were subsequently launched in the United States. In the first trial, the irinotecan/cisplatin schedule was modified in an effort to decrease toxicity, leading to equivalent response rates (48% for irinotecan/cisplatin versus 44% for EP), median time to progression (4 versus 5 months), and median OS (9 versus 10 months).425 The Southwest Oncology Group (SWOG) compared these two regimens with the same dose and schedule used in the Japanese trial and also showed, in a well-powered study, that outcomes are equivalent with the two regimens in Caucasian patients.109 High response rates have been reported in several trials using irinotecan and carboplatin with varied dosing schedules.110,111 A phase III trial comparing that regimen with etoposide/cisplatin showed improved survival, but the median survival of 7 months in the control arm, which used oral etoposide, was lower than expected.112 Many hypothesize that population-based polymorphisms in uridine 5′-diphospho (UDP)-glucuronosyltransferase (UGT1A1), the enzyme responsible for detoxifying SN-38, the active metabolite of irinotecan, may account for differences in toxicity and efficacy between Japanese and Americans.113 The regimen of topotecan plus cisplatin also has undergone phase II and III testing.114,115 Eckardt et al.115 reported the results of a randomized trial including 784 patients in which patients received oral topotecan (1.7 mg/m2 per day for 5 days) plus cisplatin, or standard etoposide and cisplatin. The response rates, median survival, and 1-year survival were identical. Severe neutropenia occurred more often with EP, but oral topotecan and cisplatin caused more anemia and thrombocytopenia.
Strategies to Improve Outcomes with Chemotherapy Regimens
Alternating Cycles of Combination Chemotherapy Regimens. The recognition of clonal heterogeneity within a tumor and the intolerability of treatment regimens that included more than four drugs due to overlapping toxicity led to trials of alternating chemotherapy combinations. The somatic mutation model developed by Goldie et al.116 predicted that the best probability of cure was achieved by the earliest possible introduction and the most rapid alternation of all active agents. If two equally effective non–cross-resistant regimens were available, the model predicted that alternating between regimens every other cycle would be more effective than alternating after every three cycles or giving one regimen continuously for five cycles before switching to the second regimen.
Many randomized clinical trials have tested the concept of alternating multidrug combinations.100,117–121 The fact that the EP regimen was effective in patients who had progressed after cyclophosphamide-based chemotherapy suggested that these drug combinations were non–cross-resistant.122 With this in mind, the National Cancer Institute of Canada conducted a study in which 289 patients were randomized to CAV or CAV alternating with EP.119 Chemotherapy was given for a total of six cycles. The response rate (65% versus 47%), PFS, and median survival time (10 months versus 8 months) favored the patients who had received alternating therapy. The authors postulated that these findings could be the result of the inclusion of a more active regimen (i.e., EP) within the alternating arm, an advantage due to greater drug diversity with five effective drugs rather than three, or support of the Goldie et al. concept. A Japanese study compared CAV to EP to alternating CAV/EP in 288 patients with limited or extensive stage disease.99 Patients with limited disease received four cycles of chemotherapy followed by thoracic irradiation and were found to have improved survival with the alternating regimen compared with CAV (p = 0.058) or EP (p = 0.032). No differences in survival were noted in the patients with extensive disease. Roth et al.100 evaluated 437 patients with extensive disease in a randomized trial comparing EP for four cycles, CAV for six cycles, or CAV alternating with EP for a total of six cycles. Although a slight improvement occurred in PFS (p = 0.052) with the alternating regimen, there was no difference in response rate or OS among the treatment arms. The patients whose tumors did not respond to CAV and were crossed over to EP were twice as likely to benefit as individuals who initially received EP and were crossed over to CAV, although these differences were not significant (28% versus 14% for induction responders who relapsed and 15% versus 8% for patients with primary resistance). The modest activity seen when refractory patients were crossed over from one of these regimens to the other suggests that the CAV and EP combinations are not entirely cross-resistant, which works against a primary assumption of the Goldie et al. hypothesis. Taking all of these studies together, alternating regimens appears to have slight or no benefit over initial treatment with EP alone.
Additional studies have evaluated alternating chemotherapy introduced after achieving a response to an induction regimen.123–125 The National Cancer Institute of Canada designed a randomized trial in which 300 patients with limited disease received either CAV for three cycles followed by EP for three cycles or CAV alternating with EP for a total of six cycles.126 Response rates, time to treatment failure, or survival did not differ. Wolf et al.123 randomized 321 patients to treatment with ifosfamide plus etoposide given until a response plateau, followed by CAV or ifosfamide plus etoposide alternating with CAV. A total of six cycles of chemotherapy were delivered in each arm. No difference in outcome was noted.
Studies also have evaluated alternating more intensive regimens. For example, a German multicenter trial demonstrated that an alternating eight-drug regimen was superior to CAV.127 Two other European trials testing three drugs regimens alternating with four drug regimens found no survival advantage to that approach.120,128 Again, the median survival times observed in these studies were no different from those that used EP alone.99,100
Addition of a Third Chemotherapeutic Agent to Etoposide Plus Cisplatin. All efforts to add a third drug to the standard EP regimen have resulted in more toxicity with little or no improvement in survival. The three-drug regimen of etoposide, ifosfamide, and cisplatin (VIP), developed initially for refractory germ cell tumors, also has been evaluated in SCLC.129 In randomized trials comparing VIP to EP, one study, which included patients with limited and extensive disease, found no difference in survival between the two treatment groups,130 whereas another, which was larger and enrolled only patients with extensive disease, identified a significant difference in median survival (9 months versus 7 months) and 2-year survival rates (13% versus 5%).131 In both studies, myelosuppression was more severe in the ifosfamide-containing arm. Single-arm studies substituting carboplatin for cisplatin in ifosfamide, carboplatin, and etoposide (ICE) have shown impressive response rates, yet cumulative myelosuppression.132,133 A large trial comparing ICE plus a midcycle dose of vincristine to other standard therapy demonstrated an improvement in the median and 1-year survival rates.134 However, an increased rate of septicemia was noted with ifosfamide, carboplatin, and etoposide-vincristine (ICE-V) (15% versus 7% in the control arm).
Studies that added paclitaxel to EP reach the same conclusion: enhanced toxicity with similar efficacy. Two studies that compared EP to EP plus paclitaxel showed that the addition of the third drug increased toxicity, as well as treatment-related mortality, without improving survival.135,136 A German study that added paclitaxel to etoposide and carboplatin demonstrated a significantly better median survival (13 months versus 12 months) and 3-year survival (17% versus 9%) only in patients with limited disease as compared to treatment with etoposide, carboplatin, and vincristine.137
Maintenance Therapy. A large number of randomized studies have examined whether maintenance chemotherapy prolongs survival in SCLC.117,138–148 Three studies that randomized patients in complete remission after induction therapy to maintenance treatment or observation identified improved survival with the prolonged treatment program in some patient groups.117,141,144 The Cancer and Leukemia Group B (CALGB) randomized 258 patients to one of four chemotherapy regimens, and 57 patients in complete remission underwent a second randomization to maintenance therapy or observation. Among the 46 patients with limited disease who proceeded to the second randomization, the median survival was improved with maintenance chemotherapy (17 months versus 7 months).144 However, the initial regimens used in this study might be considered inferior to currently used treatments. In a second study, patients treated with six cycles of CAV and in complete remission were randomized to six additional cycles of the same chemotherapy or observation.141 For the patients with extensive disease, the median survival was improved by approximately 4 months with maintenance treatment. In an ECOG trial, patients were randomized to CAV alternating with another three-drug combination or CAV alone and, subsequently, those in complete remission after six to eight cycles of induction underwent a second randomization to maintenance treatment or observation.117 Patients assigned to CAV and maintenance therapy had a longer PFS and OS (p = 0.09) than patients who received only CAV with no maintenance. In contrast, for the patients who received the six-drug regimen, those who were given no maintenance survived longer than the patients who received maintenance treatment. These studies suggest that there may be patients—perhaps those with particularly chemotherapy-sensitive disease—who derive a benefit from maintenance. In unselected patients, however, clinical trials that have evaluated treatment programs that extend beyond six cycles of chemotherapy have not demonstrated an advantage in survival.
The Medical Research Council randomized 265 patients who had responded to six cycles of induction chemotherapy to an additional six cycles of maintenance or observation.138 Overall, there was no difference in survival between patients treated with 6 or 12 cycles of chemotherapy, although for patients in complete remission at the time of randomization, a subset analysis suggested that maintenance provides a survival benefit. Three other large studies that randomized patients responding to 5 or 6 cycles of induction to a total of 12 cycles of chemotherapy or observation found no difference in outcome.142,143,146 Another study that randomized patients with limited disease from the start of chemotherapy to a total of 6 or 12 cycles identified inferior survival in the arm treated with the longer course of therapy.140
Other studies have evaluated whether four cycles of chemotherapy are adequate.139,145,149 Spiro et al.149 designed a study that included a double randomization at diagnosis. Patients received four or eight cycles of CEV and on relapse were given additional chemotherapy or supportive care. Of the four treatment arms, patients who received four cycles of chemotherapy and only supportive care at relapse had a significantly inferior median survival of 30 weeks. Four cycles of treatment were found to be adequate, provided that chemotherapy was offered to patients appropriate for additional therapy at relapse. Two additional studies evaluated four cycles of induction with longer treatment programs. A European trial randomized patients with limited and extensive disease who responded to four cycles of EP to CAV for up to 10 additional cycles or to observation with no survival differences, although the study had limited power due to small sample size.139 ECOG enrolled 402 eligible patients with extensive-stage disease into a trial that delivered four cycles of EP followed by a randomization of patients with at least stable disease to four additional cycles of topotecan or to observation.145 Although maintenance therapy increased the time before documentation of disease progression, there was no difference in OS.
Two recent meta-analyses have been conducted evaluating maintenance chemotherapy showing small improvements in survival and an increase in toxicity.150,151 Bozcuk and colleagues150 reported an improved 1- and 2-year survival by 9% and 4%, respectively. Although Rossi et al.151 showed a significant OS benefit (hazard ratio [HR], 0.89, 95% confidence interval [CI], 0.81 to 0.92; p = 0.02) for maintenance treatment, this improvement was projected to an additional 2 weeks.151 Further, there was a high heterogeneity among the included trials.
In summary, four to six cycles of chemotherapy appear to be optimal in the management of limited and extensive SCLC. After the completion of this initial treatment, patients should be monitored closely and then offered further chemotherapy at the time of progression. Both the NCCN and the European Society of Medical Oncology Guidelines support this approach.52,152
Dose Intensification. In experimental models, numerous chemotherapy drugs display log-linear or near linear dose-response curves,153 and high-dose chemotherapy has proven effective at treating hematologic diseases. It seemed reasonable to test the hypothesis that more intensive chemotherapy could improve outcomes in SCLC. Methods used have included the use of higher chemotherapy doses without or with hematopoietic growth factor support, shortened cycle length, or extreme dose intensification with marrow or peripheral blood stem cell support.
Several investigators evaluated whether increasing the dose of drugs beyond the usual dose improves survival.154–159 Three randomized trials comparing standard versus high-dose CAV156,158 or EP157 found no difference in response rates or median survival. No hematopoietic growth factors were used in these three trials, and, as such, myelosuppression and infections were significantly more severe in the high-dose arms. A randomized trial that did utilize granulocyte-macrophage colony-stimulating factor (GM-CSF) with dose escalation found that excess toxicity actually resulted in lower drug delivery and poorer response and survival rates in the dose-intense arm.159 Only a French study with 105 limited-stage patients demonstrated improvements in PFS at 2 years (28% versus 8%) and OS (43% versus 26%) with the administration of higher drug doses.154 Few oncologists have embraced this approach.
A number of studies have evaluated whether shortening the interval between chemotherapy cycles improves survival. A multicenter study randomized 300 patients, mostly with limited-stage disease, to six cycles of ICE-V delivered every 4 weeks or every 3 weeks.160 In a second randomization, patients were given GM-CSF or placebo after each chemotherapy cycle. The delivered dose intensity was increased by 26% in the group receiving chemotherapy every 3 weeks compared to those treated every 4 weeks. The median survival (443 days versus 351 days) and the 2-year survival rate (33% versus 18%) were better in the intensified arm (p = 0.0014). GM-CSF did not reduce the incidence or the duration of febrile neutropenia, and there was no difference in survival between the patients who received GM-CSF or placebo. In a subsequent study, ICE given every 4 weeks was compared to ICE given every 2 weeks with support of GM-CSF, and autologous blood collected before the cycle was reinfused 24 hours after the chemotherapy.161 Although the median delivered dose intensity was increased by 82% without significant increased toxicity, no survival benefit was identified. Two studies compared treatment with cyclophosphamide, doxorubicin, and etoposide given either every 3 weeks, or every 2 weeks with GM-CSF support.162,163 The larger trial,163 which also included a higher percentage of limited-stage patients, showed an improvement in complete response rate and OS, but the other trial did not. No fewer than four randomized trials have shown that intensive multidrug weekly regimens are no better, yet significantly more toxic than standard regimens.164–167
Numerous reports cite the use of high-dose chemotherapy with autologous bone marrow or stem cell rescue for treating SCLC.168–186 These studies have included small numbers of highly selected patients.161,182,183,187–189 Survival has not been shown to be better than conventional treatment. As in other chemosensitive solid tumors like breast cancer, high-dose chemotherapy with stem cell support does not appear to have a role in SCLC.
Treatment After Relapse Following Initial Therapy. The strongest predictor of outcome for patients with relapsed SCLC is the duration of remission. As such, patients are distinguished as having sensitive or refractory disease. The term sensitive implies an appropriate response to initial therapy that is maintained for 3 months or more. These patients have a higher likelihood of response to any additional chemotherapy; although, at best, it is approximately half that expected in the first-line setting. Survival from the start of a second regimen averages around 6 months. Patients with refractory disease either had no response to initial therapy or progressed within 3 months after completing treatment. Their chance of response to additional therapy is less than 10%, and their median survival from the start of a second regimen is 4 months.
The only approved agent in relapsed disease is topotecan. Ardizzoni et al.190 reported a phase II trial in which topotecan, administered at a dose of 1.5 mg/m2 daily for 5 days, yielded a response rate of 38% in sensitive patients and 6% in refractory patients. Median survival from the start of second-line therapy was 7 and 5 months, respectively. A randomized trial compared topotecan, administered at that same dose and schedule, to CAV in patients who relapsed at least 2 months after initial therapy.191 The response rates for topotecan (24%) and for CAV (18%) were similar. The median survival was 6 months in both arms. Symptom improvement was better with topotecan for four of the eight symptoms queried, and as such, the U.S. Food and Drug Administration approved intravenous topotecan for sensitive relapsed SCLC. Oral topotecan has also undergone extensive testing in patients with relapsed SCLC. In a randomized phase II study, oral topotecan at a dose of 2.3 mg/m2 daily for 5 days was comparable to intravenous topotecan 1.5 mg/m2 daily for 5 days with regard to response rate (23% versus 15%), median survival (32 weeks versus 25 weeks), and symptom control.192 Subsequently, the Medical Research Council showed that oral topotecan improved survival in relapsed sensitive and refractory SCLC over best supportive care alone (26 versus 14 weeks, respectively).193 Oral topotecan led to a response rate of 7%, with a slower deterioration of quality of life and symptomatology. Another phase III study randomized 309 SCLC patients who had relapsed ≥90 days after first-line therapy to receive oral topotecan or intravenous topotecan.194 The overall response rate and median survival time were 18.3% and 33 weeks, respectively, for patients who received oral topotecan compared to 21.9% and 35 weeks, respectively, for those who received intravenous topotecan. Although oral topotecan was associated with a lower incidence of grade 4 neutropenia, diarrhea occurred more often in this group of patients. Oral topotecan also has received regulatory approval for second-line therapy of SCLC.
Amrubicin, a third-generation synthetic 9-amino-anthracycline with diverse molecular effects including DNA intercalation, inhibition of topoisomerase II, and stabilization of topoisomerase IIa cleavable complexes, has been studied extensively and has received approval in Japan for SCLC treatment.195 A randomized phase II trial conducted there showed higher response rates and PFS compared with topotecan.196 Two North American phase II trials of amrubicin showed encouraging results.197,198 In patients with refractory SCLC, the overall response rate for single-agent amrubicin was found to be 21%, with median PFS and OS of 3.2 and 6 months, respectively. Subsequently, 76 patients with sensitive SCLC were randomized in a 2:1 fashion to receive amrubicin or topotecan. Amrubicin treatment resulted in a significantly higher response rate than topotecan (44% versus 15%, p = 0.021), which led to improved PFS (4.5 versus 3.3 months) and OS (9.2 versus 7.6 months).198 Despite phase II activity, preliminary results of the phase III study, which compared amrubicin to topotecan, were disappointing.199 Although the activity of amrubicin was apparent, there was no statistically significant difference in OS observed between the two arms. The trend favored amrubicin (HR, 0.82; 95% CI, 0.68 to 0.99; p = 0.036), especially in the subgroup of patients with primary refractory disease (HR, 0.77; 95% CI, 0.59 to 1.0; p = 0.047). Although lower hematologic adverse events were noted in the amrubicin arm, these patients had a higher incidence of infections. The role of amrubicin for the treatment of patients with relapsed SCLC remains to be defined.
Temozolomide is an oral alkylating agent that crosses the blood–brain barrier. A phase II clinical trial of temozolomide in 64 patients with relapsed sensitive or refractory SCLC has been performed.200 Temozolomide therapy was well tolerated and associated with an overall response rate of 20% in this patient population, with a 23% response rate in the sensitive group (n = 48) and a 13% response rate in the refractory cohort (n = 16). Responses also were noted in patients receiving temozolomide as third-line treatment and in those with brain metastases.200 There is an ongoing multicenter phase II study comparing temozolomide and veliparib (a poly [ADP-ribose] polymerase [PARP] inhibitor) versus temozolomide and placebo in patients with relapsed sensitive and refractory SCLC (ClinicalTrials.gov identifier: NCT01638546).
Multiple trials have been conducted using other agents in this patient population. A list of single agents and their activity in relapsed SCLC is found in Table 42.2, many of which also have been tested in combination studies. In summary, the optimal drug or combination of drugs in relapsed SCLC has not been established. Single-agent topotecan or CAV are appropriate for patients with sensitive relapse. These regimens also could be used for patients with refractory SCLC, although the response rates are lower. Agents evaluated in phase II trials with activity in SCLC can be considered. For patients with relapse 6 months or more after initial therapy, rechallenging with the same regimen as used in first-line treatment is also a consideration.52
Immunotherapy and Other Targeted Therapies
In light of the therapeutic plateau achieved with current chemotherapy, investigators have studied a wide range of novel therapies in the hopes of improving outcomes (Table 42.3).
Receptor Tyrosine Kinases and Growth Factors. Small molecule kinase inhibitors are now established therapies for several diseases, but as yet, have not proven efficacious in SCLC. c-Kit protein expression has been reported in 28% to 93% of SCLC tumors.201 In vitro studies support the role of c-kit and its ligand, stem cell factor (SCF), on SCLC autocrine and paracrine growth stimulation,202 and imatinib has demonstrated growth inhibition of multiple SCLC cell lines.203 Nonetheless, three phase II studies in SCLC failed to demonstrate a single radiologic response to imatinib, even when enrollment was restricted to patients with tumors expressing c-kit protein by immunohistochemistry.201,204,205
The PI3K/AKT/mammalian target of rapamycin (mTOR) signal pathway is defective in SCLC: SCLC cells possess a constitutively active PI3K206 and harbor PI3K and PTEN mutations22,23,207; phosphorylated AKT is present in 70% of tumors in SCLC patients208; and protein expression of mTOR, S6K1, and phosphorylated 4EBP1 are elevated in SCLC cells compared to type II epithelial cells.209 Such alterations lead to growth, survival, and chemotherapy resistance in SCLC. Temsirolimus—the small molecule inhibitor of mTOR—was evaluated in an ECOG trial in which patients were randomized after initial chemotherapy to maintenance therapy with either high-dose or low-dose temsirolimus.210 Although the PFS (1.8 months versus 2.5 months) and OS were better for the high dose arm (6.5 months versus 9.0 months), these results were no better than those observed in the previous ECOG trial of topotecan maintenance therapy,145 suggesting no added benefit from temsirolimus. Similarly, a phase II trial of everolimus in relapsed SCLC did not demonstrate antitumor activity for this agent.211
The insulinlike growth factor receptor (IGF-1R), a member of the insulin receptor subclass of receptor tyrosine kinase, is activated by the ligands IGF-1 and IGF-2 and signals mitogenic and antiapoptotic signaling pathways contributing to cellular transformation and malignant growth.208 IGF-1R and its ligand, IGF-1, are expressed at increased levels in SCLC.208 The IGF-1R activates the PI3K-AKT pathway in SCLC, playing a role in the development and growth of the disease, as well as resistance to chemotherapy.208 Therefore, targeted inhibition of IGF-1R represents an attractive approach to enhancing chemotherapeutic efficacy and inhibiting tumor recurrence in patients with SCLC. Yet, the ECOG 1508 phase II study evaluating the monoclonal antibody, cixutumumab, together with cisplatin and etoposide in a randomized trial, failed to show an improvement in PFS with IGF-1R inhibition.212
Developmental Pathways: The Hedgehog Pathway. The Hedgehog pathway is essential in early lung development and has a role in regulating stem cell maintenance and differentiation.213 Hedgehog signaling may play a significant role in the development and proliferation of SCLC, which is a relatively undifferentiated airway epithelial tumor that may recapitulate aspects of early lung development.214,215 In vitro and in vivo studies have demonstrated that Hedgehog antagonists can inhibit SCLC and, when administered following chemotherapy, such inhibition may delay or prevent the recurrence of residual disease.215 The ECOG 1508 phase II randomized trial in patients with extensive stage disease included an arm evaluating the addition of vismodegib, a Hedgehog inhibitor, to cisplatin and etoposide, which unfortunately, did not lead to an improvement in PFS.212
Nonreceptor Oncogenes: Bcl-2 Genes. The antiapoptotic gene product, bcl-2 protein, is expressed in 80% to 90% of SCLC tumor samples and, as such, is a potential therapeutic target.216,217 Oblimersen (G3139) is an antisense oligonucleotide that suppresses bcl-2 expression. The CALGB conducted a series of studies with oblimersen in combination with chemotherapy for SCLC.218,219 In a randomized phase II study of etoposide/carboplatin with or without oblimersen, survival was inferior in the patients receiving oblimersen (HR for OS, 2.13; p = 0.02).220 Insufficient suppression of bcl-2 by this agent may explain its lack of efficacy. Navitoclax, a selective high-affinity small molecule inhibitor of bcl-2 and bcl-xL (another antiapoptotic protein of the Bcl-2 family), resulted in dramatic tumor responses in SCLC cell line xenograft tumors as a single agent and enhanced the efficacy of standard cytotoxic agents against SCLC models.221–227 Yet, a recent phase II study of navitoclax demonstrated limited activity in patients with recurrent and progressive SCLC.228 Results of a completed phase I trial of navitoclax with first-line combination chemotherapy for SCLC are not yet available (ClinicalTrials.gov identifier: NCT00878449). A third agent, obatoclax mesylate, which is a small-molecule BH3-mimetic that exhibits binding affinity for a range of bcl-2 family members, has been evaluated in various clinical scenarios. A phase II trial of obatoclax mesylate added to topotecan did not exceed the historic response rate seen in topotecan alone in patients with relapsed SCLC.229 The phase II randomized study of carboplatin and etoposide with or without obatoclax followed by maintenance obatoclax in patients with newly diagnosed extensive stage SCLC failed to meet its primary endpoint of improved response rate for those receiving obatoclax, although there was a trend for improved PFS (6 versus 5.4 months, p = 0.084) and OS (10.6 versus 9.9 months, p = 0.052).230
Angiogenesis Inhibitors. Angiogenesis inhibitors have entered into standard clinical practice for numerous malignancies, and they are being tested in SCLC as well. Two phase III trials that tested thalidomide as maintenance therapy after first-line chemotherapy showed no significant effect on OS.231,232 Likewise, vandetanib, an oral TKI of vascular endothelial growth factor receptor 2 (VEGFR-2) and EGFR, failed to improve PFS in a randomized phase II maintenance trial.233 In all of these cases, toxicity was significantly greater in the treatment arms. Similarly, sorafenib (inhibitor of RAF; VEGFR-2,-3; platelet-derived growth factor receptor alpha [PDGFRα]) and cediranib (inhibitor of VEGFR-1, -2, -3; PDGFRβ; c-KIT) showed minimal activity for relapsed disease when evaluated as single agents, although cediranib demonstrated a promising PFS of 8 months when administered with cisplatin and etoposide in a phase I study.234–236
Sunitinib, which is known to inhibit VEGFR-1, -2, -3; PDGFRα; PDGFRβ; c-KIT; and FLT3, was evaluated in a phase II trial as maintenance treatment after chemotherapy in patients with untreated extensive-stage SCLC (CALGB 30504).237 After receiving four to six cycles of etoposide with cisplatin or carboplatin, patients were randomized to sunitinib or placebo until progression of disease. Patients in the placebo arm could cross over to receive sunitinib at the time of progression. The study met its primary endpoint of PFS after chemotherapy from the time of randomization (3.77 versus 2.3 months for sunitinib and placebo, respectively; HR, 1.53; 90% CI, 1.03 to 2.27; p = 0.037). Further, there was evidence of single-agent activity for sunitinib as maintenance therapy and at crossover, as well as a trend toward improvement in survival.237
Multiple phase II studies adding the VEGF monoclonal antibody, bevacizumab, to chemotherapy have not shown any increased risk of pulmonary hemorrhage in this cohort of patients who commonly have central tumors and have yielded favorable survival rates when compared to historical controls.238–240 A randomized phase II study evaluated cisplatin or carboplatin plus etoposide with or without bevacizumab, for four cycles followed by single-agent bevacizumab or placebo until progression or unacceptable toxicity in patients with untreated extensive stage SCLC.241 Median PFS was higher in the bevacizumab group than in the placebo group (5.5 versus 4.4 months; HR, 0.53; 95% CI, 0.32 to 0.86); however, there was no difference observed in OS, but a trend that favored placebo was noted (9.4 versus 10.9 months for bevacizumab and placebo groups, respectively; HR, 1.16; 95% CI, 0.66 to 2.04). Although no new or unexpected safety signals for bevacizumab were observed, the trend toward worse OS calls future prospects of bevacizumab into question unless a biomarker for benefit is discovered to select patients for this therapy.
Antigen-Independent Immunotherapy: Ipilimumab. Ipilimumab, a humanized immunoglobulin (Ig)G1 monoclonal antibody against cytotoxic T-lymphocyte antigen-4 (CTLA-4), has been approved for the treatment of patients with metastatic melanoma.242 By blocking the inhibitory signal provided by CTLA-4, this class of antibodies can prolong the activation and proliferation of tumor-directed cytotoxic T cells, thus promoting an antitumor immune response.243 A randomized, double-blind, three arm phase II trial in patients with untreated stage IIIB/IV NSCLC or extensive stage SCLC was performed to evaluate the efficacy and safety of paclitaxel and carboplatin with or without ipilimumab given on two dosing schedules.244 Among the 130 patients with SCLC, the phased dosing schedule, in which ipilimumab was started in cycle three of paclitaxel and carboplatin, appeared to improve immune-related PFS (median 6.4 months for the phased ipilimumab arm versus 5.3 months for the control arm (p = 0.03)), immune-related best overall response rate (71% [95% CI, 55 to 84] versus 53% [95% CI, 38 to 68]) and OS (median 12.9 months versus 9.9 months [p = 0.13]), compared to paclitaxel and carboplatin, whereas the concurrent regimen did not lead to improved outcomes.245 Ipilimumab did not potentiate the toxicities of the chemotherapy, but was associated with moderate immune-related adverse events.245 Given these favorable results, a randomized, multicenter, double-blind phase III trial comparing the efficacy of platinum/etoposide with or without ipilimumab in patients with newly diagnosed extensive stage disease SCLC, with OS as the primary endpoint, has been conducted and the results are forthcoming. (ClinicalTrials.gov identifier: NCT01450761).
As seen previously, distinct pathways contribute to the pathogenesis of SCLC, leading to its unique biology and clinical features. The therapeutic strategies employed previously to target the basic molecular and cellular changes in SCLC have not led to significant changes in the management and outcomes of the disease, thus far. However, continued, rational, target-based approaches ultimately should lead to improved survival of patients with SCLC.
Radiation
Role of Radiotherapy in Limited Disease. Despite being exquisitely chemo- and radioresponsive, neither modality alone controls all aspects of disease. The CALGB trial of the late 1980s demonstrated that 90% of patients treated with chemotherapy alone failed locally.246 The meta-analysis of Pignon and Arriagada247 provided more data to mandate thoracic radiotherapy, but a number of treatment issues remained to be determined, including sequencing of radiation with chemotherapy, early versus late radiotherapy, altered fractionation, and prophylactic cranial irradiation.
Concurrent combined modality therapy is the standard treatment for SCLC patients with limited-stage disease.52 It requires close coordination between medical and radiation oncologists. A combined modality treatment approach requires patients with an excellent performance status. Single-modality therapy may be appropriate for those who are debilitated or have serious comorbidities. If the patient’s condition improves sufficiently after the initial chemotherapy or radiotherapy, subsequent treatment with the other modality may be considered. Although gains in radiotherapy delivery and integration with PET imaging have been made, disease failure in local, distant, and sanctuary sites continue to be substantial clinical challenges.
Sequencing of Radiation with Chemotherapy. Concurrent therapy is the delivery of chemotherapy and radiation therapy throughout the same time period. Sequential therapy is the delivery of one modality only after the completion of the other, often requiring a delay to allow for adequate recovery from the initial modality. A 1992 meta-analysis evaluated trials in which more than 2,100 patients with limited-stage SCLC were randomized to receive chemotherapy alone or with chest irradiation.248 Patients given combined modality therapy had a 14% reduction in death rate and an absolute 5.4% improvement in 3-year survival compared with those who received chemotherapy alone. Both differences were highly significant. A second and independent meta-analysis reached similar conclusions.249
The trials included in the meta-analysis used cyclophosphamide- and doxorubicin-based chemotherapy, which is excessively toxic when given with concurrent thoracic radiotherapy. Therefore, individual trials used strategies such as sequential or interdigitated chemoradiation and used different chemotherapy regimens during the concurrent phases. However, the current standard chemotherapy regimen of cisplatin and etoposide can be used safely with concurrent radiotherapy.
Thoracic Radiation Dose and Fractionation. Due to the radioresponsiveness of SCLC, modest doses of radiation from 45 to 50 Gy have been used. However, with modest-dose radiation therapy there is a high rate of local failure. For example, in the Intergroup trial, the control arm of 45 Gy given once daily had a 75% rate of intrathoracic relapse.250 Therefore, higher radiation doses or intensification (i.e., acceleration) appear necessary to improve local control. A retrospective review from Massachusetts General Hospital suggested that there may be continued dose response beyond 50 Gy.251 The maximum tolerated dose of concurrent thoracic chemoradiation seems to be 45 to 51 Gy with a twice-daily approach and 70 Gy daily.252 However, the advent of highly conformal radiotherapy techniques, such as intensity-modulated radiation therapy (IMRT) and the shift away from targeting clinically uninvolved nodal stations, may lead to tolerance of higher radiation doses, as discussed in the following paragraphs.
CALGB-39808 determined that 70 Gy delivered with daily fractions of 2 Gy with concurrent chemotherapy is feasible in the cooperative group setting and was associated with a median survival of 22.4 months and acceptable rates of esophagitis and pneumonitis.253 Other CALGB trials also have used 70 Gy of thoracic irradiation with concurrent chemotherapy.254 Once-daily fractionation is more familiar for radiation oncologists and typically is more convenient for patients, although it should be noted that some patients prefer the decreased overall treatment duration with a twice-daily schedule.
SCLC appears to be an ideal neoplasm for twice-daily treatment in that it has a high growth fraction, short cell cycle time, and small-to-absent shoulder on the in vitro cell survival curve, which may allow for a reduction in long-term pulmonary toxicity while maintaining antitumor efficacy.255 Pilot studies in the late 1980s combining etoposide and platinum with twice-daily chest radiation were promising, with median survivals greater than 2 years and, in most series, low rates of pneumonitis.250,256,257 An Intergroup study randomized 417 patients with limited-stage SCLC receiving 45 Gy in either daily fractions of 1.8 Gy or twice-daily fractions of 1.5 Gy, both given concurrently with the first of four cycles of EP.49 Although fractionation is the obvious variable, the overall duration of radiotherapy varied as well (3 weeks versus 5 weeks), and longer treatment times may exert selective pressure on the emergence of resistant clones. The target volume included the primary tumor, bilateral mediastinal nodes, and the ipsilateral hilum, excluding uninvolved supraclavicular nodes. Local failure was reduced from 52% to 36% with the twice-daily schedule (p = 0.06). Of interest, only 6% of patients with twice-daily radiation failed in both local and distant sites, compared to 23% with daily treatment (p = 0.01). More importantly, although statistically significant differences in survival were not seen at 2 years,257 by 5 years the survival was 16% with once-daily treatment, compared to 26% with a twice-daily schedule (p = 0.04).49 All patients who achieved less than complete response were scored as local failures, but some of those treated with the accelerated scheme who achieved only a partial response survived, as well as those with a complete response, implying that the local failure rate was overestimated by imaging on that arm. There was a higher frequency of grade 3 esophagitis with twice-daily treatment, but overall long-term morbidities were not significantly different between the two arms.
A North Central Cancer Treatment Group trial attempted to reduce morbidity of twice-daily radiation by inserting a 2.5-week pause between two courses of 24 Gy each (therefore, the overall course was longer than the standard duration).48,258 After three cycles of induction chemotherapy, fit and responding patients were randomized to receive either the 48 Gy split-course regimen, or 54 Gy in a once daily regimen in 6 weeks.258 The 20% rate of 5-year survival was less than the benchmark 26% from the Intergroup trial. However, a follow-up trial used a higher dose of twice-daily radiation (total 60 Gy) with a 2-week treatment break and reported a favorable 5-year survival of 24%.259
A phase I trial conducted by the Radiation Therapy and Oncology Group (RTOG) and CALGB evaluated the use of 70 Gy delivered in daily fractionation or 45 Gy given in twice-a-day fractionation.260 Although it was intended to establish the maximum-tolerated doses (MTD) of irinotecan given with cisplatin and thoracic radiation, it also was the first trial to evaluate 70 Gy delivered at cycle one. Of the 15 patients treated to 70 Gy, 2 had dose-limiting toxicities (diarrhea, esophagitis, and cardiovascular complications).
RTOG-9712 was a phase I trial to establish the MTD of radiation therapy with delayed accelerated hyperfractionation.261 With this technique, a large field encompassing the gross tumor and mediastinum was treated to 45 Gy. A smaller field that encompassed only the gross tumor was treated as a second daily 1.8 Gy treatment for the last 3 to 11 days. The MTD was found to be 61.2 Gy with this regimen, which subsequently was evaluated in RTOG-0239, a phase II trial.262 It reported a 2-year OS of 37%, short of the predicted survival of 60%. However, the regimen demonstrated an excellent local control of 73%.
Currently, a randomized phase III trial is being conducted by the RTOG and CALGB to evaluate three fractionation schemes: 45 Gy in 1.5-Gy twice-daily fractions (standard), 70 Gy in 2-Gy fractions (Arm B), and 61.2 Gy with delayed accelerated hyperfractionation (Arm C). In the first part of this trial, toxicity was to be assessed and the less toxic of Arms B and C was to be compared head to head with the standard arm. Although no clear difference in toxicity was observed between Arms B and C, the delayed accelerated hyperfractionation arm has been dropped due to slow accrual, and the study is continuing as a two-arm trial. A separate Phase III randomized trial is also evaluating once versus twice-daily radiotherapy with concurrent chemoradiotherapy in Europe, comparing 66 Gy in daily 2-Gy fractions against the same control arm of 45 Gy in twice-daily 1.5-Gy fractions. Until results from these trials are available, twice-daily fractionation as established by the Intergroup trial remains the reference regimen for fit patients. However, it should be noted that the logistical and toxicity obstacles with twice-daily treatment apparently are substantial, because a recent survey of practice patterns indicated that fewer than a quarter of limited-stage SCLC patients receive twice-daily treatment in the United States.263
Early Versus Late Radiotherapy. Randomized trials have yielded conflicting results on whether concurrent irradiation is best given early or late in the chemotherapy program. There have been multiple meta-analyses of the timing of thoracic irradiation.264–268 One meta-analysis265 reviewed seven randomized trials with a total of 1,524 patients that addressed the timing of radiotherapy relative to chemotherapy. Early radiation therapy was defined as beginning before 9 weeks after the initiation of chemotherapy and before the third cycle of chemotherapy. Late radiation therapy began 9 weeks or more after the initiation of chemotherapy or after the beginning of the third cycle. They reported a small but statistically significant improvement in 2-year survival for patients receiving early radiation therapy. A greater benefit was observed in patients receiving hyperfractionated radiation. Another meta-analysis269 evaluated four randomized trials consisting of 1,056 patients to determine whether the time from the start of chemotherapy until the end of radiotherapy (SER) was a predictor of survival. They found that there was a significantly higher 5-year survival rate in the treatment arms with a shorter SER. In addition, a low SER was associated with a higher incidence of severe esophagitis. This suggests that an important factor in the treatment of SCLC involves counteracting accelerated repopulation that occurs after treatment with chemotherapy. However, definitive evidence that early integration of radiotherapy leads to improved survival remains elusive. A recent randomized trial from Korea assigned patients to receive radiotherapy (albeit a nonstandard regimen of 52.5 Gy) with either the first or third cycle of chemotherapy with cisplatin or etoposide. There was no difference in survival or local control, but rather an increase in febrile neutropenia with early radiotherapy, suggesting that later integration of radiotherapy was preferable.82
In clinical practice, it is often prudent to initiate chemotherapy immediately in these patients who are typically highly symptomatic and not delay treatment until radiation treatment planning is complete. Starting radiotherapy with the second cycle of chemotherapy is more readily achievable and should preserve the potential gains in efficacy obtained with early integration of radiotherapy with chemotherapy.
Radiation Therapy Treatment Volumes and Technique. An early randomized trial by SWOG showed no difference in recurrence rate whether pre- or postchemotherapy imaging was used to determine radiation therapy treatment fields.270 Of course, if early radiation therapy is used, then there is no postchemotherapy treatment volume. The Intergroup trial49 included gross disease, the bilateral mediastinum, and the ipsilateral hilum in the treatment field. The uninvolved supraclavicular area was excluded. RTOG-9712261 allowed for the treatment of the uninvolved supraclavicular area in the setting of apical tumors. A small phase II trial suggested that there may be increased elective nodal failure in the supraclavicular area if it is excluded from the treatment field.271 Consultants from the International Atomic Energy Agency reviewed available literature in 2008 and found little evidence to guide the use of elective nodal irradiation.272 However, a number of prospective and retrospective experiences have since been published and increasingly suggest that involved-field radiation therapy is not associated with an excessive rate of local–regional failure, particularly in an era of routine PET staging. A Dutch phase II trial of concurrent chemoradiation limited radiotherapy (RT) fields to the primary tumor and clinically involved lymph nodes and reported a relatively low local failure rate of 16%.273
Utilizing PET to guide the design of limited radiotherapy fields appears to reduce the probability of elective nodal failure due to the improved sensitivity of PET to detect nodal disease compared to CT alone. A follow-up trial from the same group that found a worrisome rate of elective nodal failure when utilizing involved-field RT in CT-staged patients showed that the rate of isolated nodal failure was only 3% with PET staging, compared to 11% without.274 A retrospective experience from the M.D. Anderson Cancer Center similarly showed a low rate of isolated elective nodal failure in a PET-staged cohort of patients who were treated with IMRT, a technique that gives lower incidental radiation doses to untargeted lymph node regions and, therefore, would theoretically increase the risk of elective nodal failure.275 Overall, these and other recent publications suggest that with modern staging and treatment techniques, the omission of elective nodal irradiation does not lead to an excessive rate of isolated nodal failure.276–278 Neither of the ongoing trials of daily versus twice-daily thoracic radiotherapy employ elective nodal irradiation in any of the trial arms (with the exception of mandatory coverage of hilar lymph nodes in the CALGB trial), indicating that the omission of elective nodal irradiation is increasingly considered within the standard of care for PET-staged patients.
In addition to the omission of elective nodal irradiation, another area of investigation in radiation technique is the implementation of more highly conformal delivery methods, such as IMRT or proton therapy. These techniques allow for significantly greater control of the location of radiation dose, particularly of incidental radiation dose outside of the target volume. Although this would seem to be an unequivocal advantage, theoretic concerns have persisted regarding the sensitivity of these techniques to respiratory organ motion, and the possibility that decreasing the incidental dose outside of the target volume might increase rates of regional or nodal failure. Investigators from the M.D. Anderson Cancer Center retrospectively compared outcomes with patients receiving standard three-dimensional (3D)-conformal radiation therapy and IMRT, and found no significant difference in OS or DFS.279 Proton therapy, which reduces the dose outside of the target volume more fully than is possible with any form of photon radiotherapy, has not yet been widely used in SCLC, with only one small report published so far.280 However, if the phase III trials demonstrate an advantage to higher dose radiotherapy, then IMRT and photon therapy are likely to gain in importance, because highly conformal techniques are often required to achieve high target doses while respecting dose limits to critical normal structures.
Toxicity of Radiation Therapy. The addition of chest irradiation has increased myelosuppressive, pulmonary, and esophageal complications of treatment, particularly with concurrent cyclophosphamide-based regimens.281–283 Esophagitis is a difficult toxicity to compare because trials often use unique grading systems. However, most trials with concurrent chemoradiation with a cisplatin-based regimen report a 10% to 25% rate of severe esophagitis.284 A retrospective review revealed that various radiation dosimetric parameters, such as mean esophageal dose and volume of esophagus receiving 15 Gy, were associated with a higher incidence of grade 3 or worse esophagitis in patients receiving twice-daily radiation.285 More recently, a large individual patient data meta-analysis of esophagitis after concurrent thoracic chemoradiotherapy indicated that the best predictor of esophagitis was the volume of esophagus receiving greater than or equal to 60 Gy, with the highest risk seen when 17% or more of the esophagus was exposed to such doses.286
Radiation pneumonitis (RP) has not been as well studied in SCLC as it has in NSCLC, most likely due to the fact that most trials have used a moderate dose of radiation therapy, below which high rates of RP rarely are seen. Recent trials report a RP rate of approximately 10%.253,287 This is lower than some of the trials reported in the 1980s and 1990s, probably due to improved radiation therapy techniques and better distinction between pneumonitis and other etiologies of respiratory distress, such as infection or tumor recurrence. The volume of lung receiving 20 Gy (V20) is a standard parameter used to predict lung toxicity in patients with NSCLC. A recent collaborative effort to define consensus dose limits for RP recommended that the V20 be kept below 30% to 35% in order to keep the risk of pneumonitis less than 20%.288 It has been shown to have value in patients receiving concurrent accelerated hyperfractionated treatment for SCLC as well, with a V20 less than 25% associated with a lower rate of RP.289
Role of Chest Irradiation in Extensive Disease. Reviews of the historical literature indicated that the addition of chest irradiation plus chemotherapy for patients who have extensive-stage SCLC may improve local control in the thorax, but without change in survival.290,291 Successive large studies by the SWOG also confirmed a benefit on local control but not survival.118,292 Because patients with extensive disease generally achieve complete response rates of only 20% to 25% with current chemotherapy regimens and frequently relapse in distant metastatic sites, it is unsurprising that the routine application of additional local therapy did not have a clear impact on survival. Several clinical trials have randomized patients with extensive disease to chemotherapy alone or in combination with irradiation to the chest disease, as well as to some or all sites of overt distant metastases.292–295 Although most of these did not show survival advantages with the addition of radiotherapy, it is notable that the most recent trial did.293 In this trial, patients with at least a partial response to chemotherapy at the primary site and a complete response in distant sites were randomized to receive thoracic radiation with additional chemotherapy, or chemotherapy alone. Thoracic radiotherapy was associated with significantly better survival and a trend toward better local control. A recent, small phase II trial of consolidative thoracic radiation suggested that rates of symptomatic recurrence in the chest were low with this strategy and may, therefore, have an important quality of life benefit irrespective of any survival benefit.296 Preliminary results from the Dutch phase III trial randomizing extensive stage SCLC patients who have had a response to four to six cycles of chemotherapy to thoracic radiation therapy or no thoracic radiation therapy has found a survival benefit at two years but not at one year, which was the primary endpoint.297
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


