Radiologic Imaging Concerns
Jeffrey A. Bennett
Cancer of the nasopharynx is staged differently than other pharyngeal primaries in that more emphasis is placed on tumor extension to other spaces than on size. Therefore, it is critical that imaging clearly shows the full extent of the primary lesion. As with other mucosal tumors, endoscopy can show the mucosal extent of the tumor very well, but deep tumor invasion requires imaging. Extension to the nasal cavity or oropharynx as well as parapharyngeal invasion classifies the tumor as T2 (Fig. 22-6). A T3 lesion involves bony structures and/or the paranasal sinuses. The tumor is upstaged to T4 if there is intracranial extension, involvement of the cranial nerves, the infratemporal fossa, the hypopharynx, the orbit, or the masticator space (Fig. 22-7). Because of the importance of detecting soft tissue invasion, intracranial extension, and perineural spread, magnetic resonance imaging (MRI) is preferred to computed tomography (CT) for imaging of nasopharyngeal cancers.1,2,3,4 However, care must be taken with fat suppression as this often produces artifacts at air-bone interfaces at the skull base. CT is not without benefit as it is very good at showing cortical bone erosion.
Usually, the diagnosis of nasopharyngeal cancer is known at the time of imaging, but occasionally it is found incidentally when imaging patients with unilateral serous otitis media and Eustachian tube dysfunction, otalgia, sore throat, or cranial neuropathies. When a tumor is discovered, it is essential to describe its pattern of spread and full extent so that the patient can be correctly staged and treated appropriately. Often both CT and MRI are obtained and these certainly give complementary information. Usually, the neck is scanned with CT to evaluate lymphadenopathy as the addition of a neck MR adds significant time and expense to the MR study. Suggested protocols are given in Figures 22-8 and 22-9.
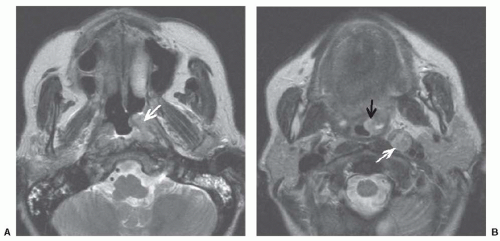 FIGURE 22-6. A: Axial T2-weighted MR image shows an infiltrating mass (arrow) in the left nasopharynx which has expanded the torus tubarius and obstructed the Eustachian tube orifice. No extension is seen into the parapharyngeal space fat. B: Axial T2-weighted MR image inferior to shows extension of tumor along the lateral pharyngeal wall into the oropharynx (black arrow). This stages the tumor as T2a. A positive left lateral retropharyngeal lymph node is well demonstrated (white arrow). |
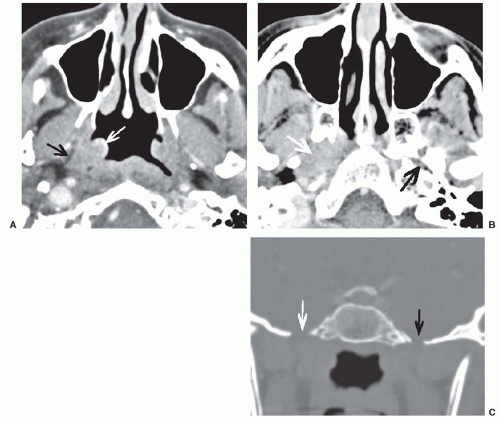 FIGURE 22-7. A: Axial postcontrast CT scan shows a right nasopharyngeal mass (white arrow). Note the preservation of fat in the parapharyngeal space deep to the pharyngobasilar fascia (black arrow). B: Axial postcontrast CT at the level of the temporomandibular joints shows that the tumor has spread superiorly (white arrow) and has destroyed bone at the petrous apex in the region of the foramen lacerum. Note the normal foramen lacerum on the opposite side (black arrow). C: Coronal reformat of the CT scan with bone windows shows enlargement of the right foramen ovale (white arrow) compared with the normal left foramen ovale (black arrow). At this point, an MRI would be warranted to look for more proximal spread of tumor along V3 to the trigeminal ganglion. |
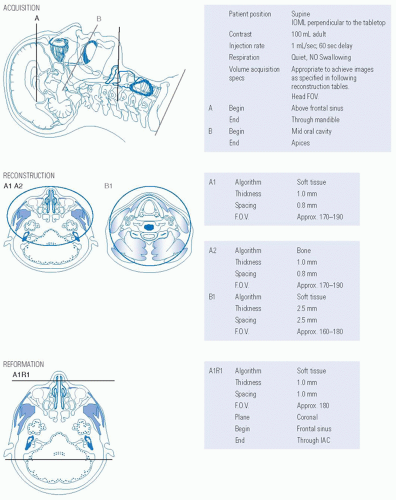 FIGURE 22-8. Protocol for CT maxillofacial detail and neck with intravenous contrast.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|