up to 100 times elevated risk of developing tumors in the upper aerodigestive tract as compared with nonsmoking, nondrinking individuals. In addition to potentiating the effects of tobacco, a moderate to high consumption of alcohol can put nonsmoking individuals at a higher risk for hypopharyngeal and cervical esophageal cancers (Table 19.1).7,11 Alcohol appears to have a stronger neoplastic effect in the hypopharynx than in the larynx, and dark liquor may carry a higher risk than light liquor.12 In addition to tobacco and alcohol, gastroesophageal reflux, obesity, and achalasia can lead to higher rates of esophageal cancer.
TABLE 19.1 Odds Ratios for Oral and Pharyngeal Cancers Associated with Alcohol Consumption. Odds Ratios (or) Adjusted for Smoking, Age, and Race | ||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||
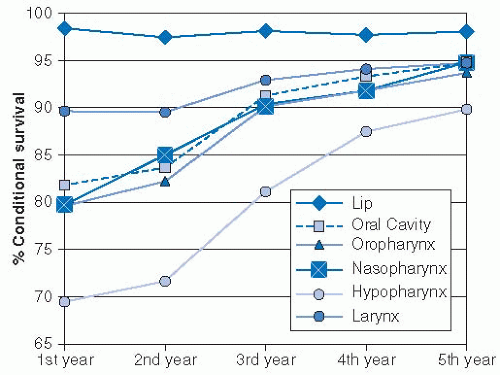 FIGURE 19-1. Conditional 5-year survival of head and neck cancers. A nearly 30% difference exists in survival through the first year, with hypopharynx cancers faring the poorest. Hypopharyngeal cancer patients continue to have lower rates of survival in years 2 to 5; secondary malignancies and comorbidities contribute to this phenomenon. Source: Reprinted with permission from Cooper JS, Porter K, Mallin K, et al. National Cancer Database report on cancer of the head and neck: 10-year update. Head Neck. 2009;31:748-758. |
HPV-negative counterparts, HPV-positive and HPV-negative esophageal cancer patients have been shown to have similar clinical risk factors.23 Therefore, although current data are suggestive of a carcinogenic role for HPV in the hypopharynx and the cervical esophagus, prospective studies demonstrating that persistent HPV infections result in malignant transformation, such as those performed in uterine cervix cancer, may be necessary to confirm this suspicion.
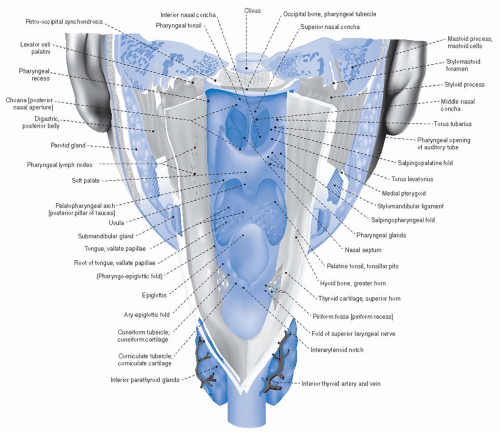 FIGURE 19-2. Posterior view of the larynx and hypopharynx as viewed by a posterior midline incision through the posterior pharyngeal wall, cricopharyngeus, and cervical esophagus. Source: From Sobotta, Atlas der Anatomie des Menschen © Elsevier GmbH, Urban & Fischer Verlag München, with permission. |
fold, and the medial, anterior, and lateral walls narrowing inferiorly to form the apices, which extend slightly below the cricoid cartilage. The pyriform sinuses are open posteriorly and contiguous with the posterior pharyngeal walls. The internal branch of the superior laryngeal nerve pierces the thyrohyoid membrane, which surrounds the superior aspects of the pyriform sinuses laterally. Tumor involvement of the sensory component of this nerve, which synapses superiorly with the nerves of the external auditory canal in the jugular ganglion, can result in referred otalgia. The remaining sensation in this region is provided by nerve fibers of the glossopharyngeal nerve. The recurrent laryngeal nerve provides motor function to the cricopharyngeus muscle and the posterior cricoarytenoid muscles of the larynx, with remaining primary motor supply to the hypopharynx provided by the pharyngeal plexus.
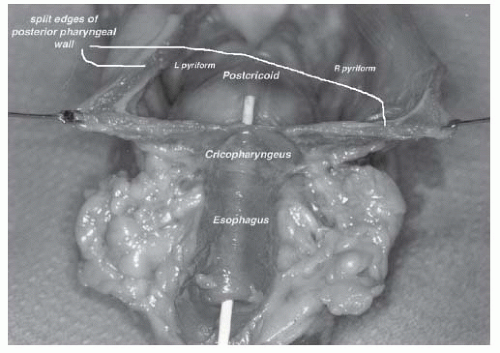 FIGURE 19-3. This anatomic specimen (with the posterior pharyngeal wall incised) allows a posterior view of the hypopharynx, demonstrating the three primary anatomic subsites (posterior pharyngeal wall, postcricoid region, and pyriform sinuses) of the hypopharynx. |
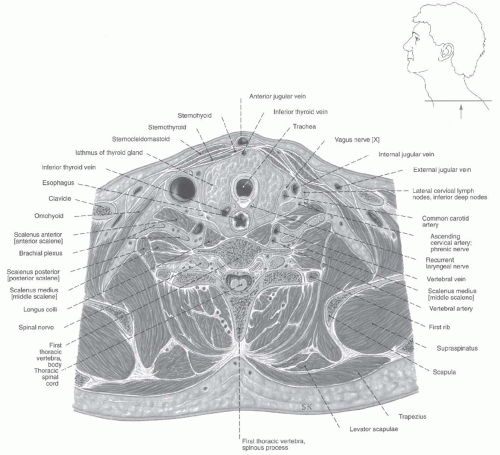 FIGURE 19-4. Transverse section detailing relationship of the cervical esophagus and adjacent structures at the level of the first thoracic vertebrae. Source: Adapted from Sobotta, Atlas der Anatomie des Menschen © Elsevier GmbH, Urban & Fischer Verlag München, with permission. |
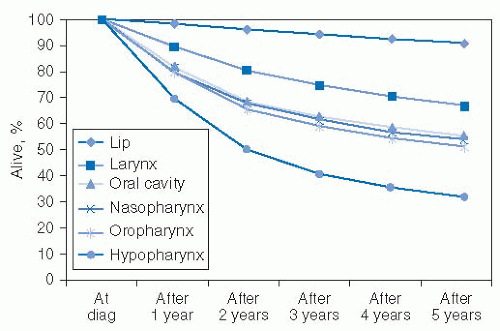 FIGURE 19-5. Five-year survival by mucosal site for head and neck cancers from 1990 to 1999 cases. Source: Reprinted with permission from Cooper JS, Porter K, Mallin K, et al. National cancer database report on cancer of the head and neck: 10-year update. Head Neck. 2009;31:748-758. |
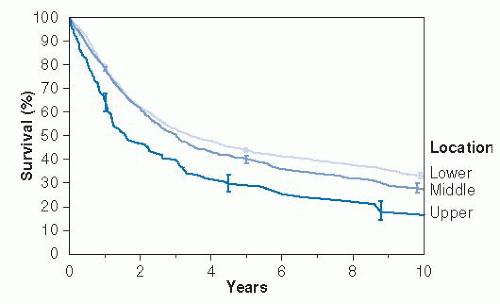 FIGURE 19-6. Survival according to upper extent of cancer in the esophagus. Source:Reprinted with permission from Rice TW, Rusch VW, Apperson-Hansen C, et al. Worldwide esophageal cancer collaboration. Dis Esophagus. 2009;22:1-8. |
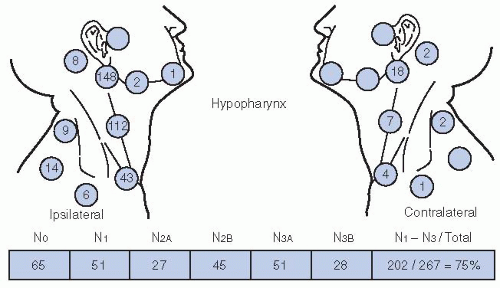 FIGURE 19-7. Nodal distribution patterns for a series of 267 patients with hypopharynx cancer as summarized by admission records at the MD Anderson Hospital. Source: Redrawn with permission from Lindberg R. Distribution of cervical lymph node metastases from squamous cell carcinoma of the upper respiratory and digestive tracts. Cancer. 1972;29:1446-1449. |
often as a result of progressive tumor-associated dysphagia and odynophagia. An assessment should be made of the patient’s nutritional status, with attempts to correct nutritional deficits prior to the initiation of aggressive therapy. A nutritionist should be involved as a part of the multidisciplinary team. A percutaneous enteral gastrostomy (PEG) tube is commonly utilized. In surgical patients, a PEG tube is commonly placed at the time of surgery to allow for maintenance of nutrition during the postoperative recovery period. Whether upfront PEG tube placement should occur routinely in patients planning to undergo (chemo)radiation or should happen only in patients who demonstrate significant difficulties with maintaining weight and hydration during radiation is an area of debate. Patients with tumors of the hypopharynx and cervical esophagus tend to have more dysphagia, odynophagia, and prediagnosis weight loss than other HNSCC patients. Therefore, in our experience, the benefits of prophylactic PEG tube placement in terms of improved weight preservation and maintenance of hydration appear warranted for the majority of patients. Therefore, we routinely place PEG tubes during the pretreatment evaluation phase prior to chemoradiation.
TABLE 19.2 Workup and Pretreatment Evaluation for Patients with Tumors of the Hypopharynx and Cervical Esophagus | ||||||||
|---|---|---|---|---|---|---|---|---|
|
TABLE 19.3 Impact of FDG-PET on Staging and Management in 233 HNSCC Patients | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||
occupy a region likely to receive high-dose radiation. Upfront removal of such teeth in poor repair is preferable to subsequent removal following radiation, as manipulation of the teeth and sockets following radiation places patients at risk for osteoradionecrosis. Dental extractions should precede radiation by 10 to 14 days to allow for adequate healing. For patients who have teeth that will remain in place through radiation should receive custom fluoride carrier trays. Long-term use following radiotherapy of fluoride can minimize dental decay in the setting of postradiotherapy xerostomia.
TABLE 19.4 T and N Staging for Esophageal Squamous Cell Carcinoma | ||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||
or pharyngolaryngoesophagectomy. However, in recent years, increasing efforts toward organ preservation have become more prevalent. As tumors of the hypopharynx and cervical esophagus tend to present with locally advanced and/or node-positive disease, these efforts at organ preservation most commonly involve chemoradiation for locally advanced disease (Fig. 19-8). However, more advanced surgical techniques may allow for organ preservation in those patients who present with early-stage disease amenable to larynx-sparing surgery. Nonetheless, radical surgery remains an important component of management and should be considered as an alternative to organ-sparing approaches, depending on the motivation of the patient for organ preservation and the patient’s medical comorbidities. Active rehabilitation therapy in order to maximize eventual speech and swallow function must accompany all definitive management, regardless of the specific treatment approach. Rehabilitation and posttreatment surveillance are discussed at the end of this section.
TABLE 19.5 Stage Grouping for Esophageal Squamous Cell Carcinoma | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


