Radiologic Imaging Concerns
Jeffrey A. Bennett
Imaging the larynx requires high speed because of the difficulties patients have with secretions and throat discomfort, which lead to frequent swallowing, coughing, and resultant motion artifact. Therefore, computed tomography (CT) is the imaging modality of choice, especially with the newer multidetector row helical or volumetric scanners. Very thin axial sections can be obtained, down to 0.5 mm, which allow outstanding quality of sagittal and coronal reformats. The axial images should be performed parallel to the true vocal cords to allow the best view of the anterior and posterior commissures. However, this is proving to be less important now, because many PACS software packages allow reformation of the images in any plane. This data manipulation can essentially “straighten out” the patient and optimize the imaging plane, no matter how the images were acquired. The long imaging time required for magnetic resonance imaging (MRI) often results in motion-degraded images, but in cooperative patients who are able to hold very still and not swallow for extended periods of time, MRI still provides better soft tissue differentiation. Since this scenario is infrequent, MRI is mostly reserved for problem solving in more advanced transglottic tumors, such as when there is a question of tracheal or esophageal invasion. Intravenous contrast is necessary for both modalities. Suggested protocols are given in Figures 18-9 and 18-10.
No matter which imaging technique is chosen, MRI or CT, the information obtained is critical in staging.1 Imaging frequently upgrades clinically suspected low-grade tumor based on submucosal spread deep to the mucosal lesion visualized with endoscopy. As seen elsewhere in the head and neck, visualization of fat planes is critical to image interpretation (Fig. 18-11). In the larynx, obliteration of the paraglottic fat and preepiglottic fat are signs of tumor extension. At the level of the true vocal cords, normally no fat is seen in the paraglottic space, but at the level of the false cords a clear paraglottic fat plane should be seen. The anterior commissure is very thin, and normally minimal to no soft tissue should be seen at that location. Similarly, in the subglottic region, no soft tissue should be seen in the airway inside the cricoid cartilage. Soft tissue in these locations is a sign of tumor spread. Multiplanar imaging is helpful for determining the full extent of the primary tumor (Fig. 18-12).
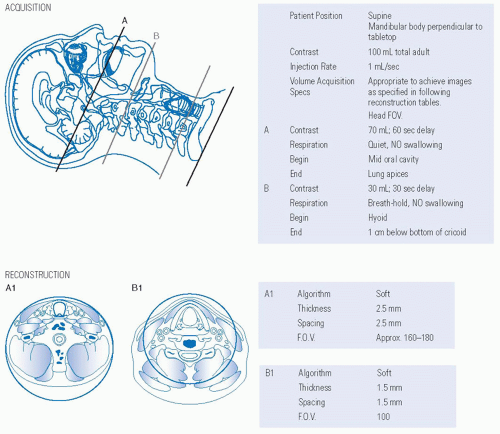 FIGURE 18-9. Protocol for CT scan of the larynx with intravenous contrast. CT, computed tomography. Source: Reprinted from Mancuso AA, Hanafee WN. Head and Neck Radiology. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:2222, with permission. |
Occasionally, gross morphologic changes to the larynx such as a laryngocele are caused by a tumor. A careful search for an obstructing mass should be performed when a laryngocele is encountered (Figs. 18-13 and 18-14).
Not uncommonly, the laryngeal cartilages will be seen to be sclerotic. There is frequently irregular ossification of the laryngeal cartilage, so asymmetries cannot be assumed to be tumor invasion of the cartilage. The best way to be sure that cartilage invasion has occurred is if tumor is seen on both sides of the cartilage (Fig. 18-15). The arytenoid cartilage is frequently sclerotic. Pathologic studies have revealed a 50% likelihood of microscopic cartilage invasion in a single sclerotic cartilage directly adjacent to the tumor. There is a >90% possibility of cartilage invasion if more than two adjacent cartilages are sclerotic next to the tumor. Cartilage sclerosis has been correlated with a poorer local control rate with radiation therapy.2 Both CT and MRI can detect cartilage sclerosis, appearing solid bright on CT and black on MRI. Initial studies reported a higher specificity for cartilage invasion with CT compared to MRI.3 A recent study was performed4 to investigate the accuracy of MRI in predicting thyroid cartilage invasion and found that MRI overpredicts cartilage and thyroid gland invasion.
Examples of glottic squamous cell carcinoma spreading to the supraglottis and subglottic region are given in Figures 18-16, 18-17 and 18-18.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


