Radiologic Imaging Concerns
Jeffrey A. Bennett
Thyroid nodules are detected frequently on physical examination and are found even more commonly on imaging studies of the neck, including computed tomography (CT), magnetic resonance imaging (MRI), and ultrasound, performed for reasons other than evaluation of the thyroid gland. There remains controversy over how to manage these nodules as their initial workup and surveillance poses a considerable economic burden on society, and the vast majority of the lesions will never pose a threat to the patient’s life. Ultrasound is the main imaging modality used to evaluate and triage lesions for biopsy and/or follow-up. Recommendations have been made concerning imaging features that suggest a nodule might be biopsied or followed, depending on the clinical scenario.1,2,3,4,5,6,7,8 If a nodule is >75% cystic, it is probably benign. Nodules <1 cm in diameter are usually not biopsied. A dominant nodule that is >1 cm in diameter and is >25% solid is usually biopsied. Other ultrasound features that suggest malignancy are nodules with central rather than peripheral hypervascularity and nodules with irregular margins. Palpable nodules can be biopsied without image guidance. Ultrasound guided biopsies are performed when the nodule is not palpable (Fig. 28-16). Biopsy is almost always performed with fine-needle aspiration. A 25 or 27 gauge needle should be used as larger needles produce inferior samples with more blood.
New techniques in ultrasound are now being applied to the evaluation of thyroid nodules. Acoustic radiation force impulse imaging is being used to evaluate the elasticity of nodules. Two methods termed Virtual Touch tissue imaging and Virtual Touch tissue quantification (Siemens Medical Solutions, Mountain View, CA) have shown the elastic parameters of malignant nodules to be significantly higher than those of benign nodules.9 It remains to be determined whether this type of imaging can reduce the need for fine-needle aspiration.
Nuclear medicine imaging studies with radioactive iodine rarely help in the workup of asymptomatic thyroid nodules. They can aid in the determination of which nodules should be biopsied
in the patient with multiple nodules, as cold nodules are three times more likely than other nodules to be cancer. Radioactive iodine studies are used often for follow-up of papillary and follicular cancer, but not all cell lines are or remain iodine avid. Thallium-201 has been used as a general tumor marker for thyroid cancer. Octriotide nuclear scanning is useful for detecting and staging medullary thyroid cancer. FDG-PET is also used for evaluation of recurrent thyroid cancer, usually in the scenario where despite a rising thyroglobulin level, iodine-131 scan does not show activity. These iodine negative metastases are better detected with FDG-PET.10 FDG-PET is also useful for more aggressive biologically active tumors such as medullary and anaplastic cancers and remains useful for the detection of distant metastases.
in the patient with multiple nodules, as cold nodules are three times more likely than other nodules to be cancer. Radioactive iodine studies are used often for follow-up of papillary and follicular cancer, but not all cell lines are or remain iodine avid. Thallium-201 has been used as a general tumor marker for thyroid cancer. Octriotide nuclear scanning is useful for detecting and staging medullary thyroid cancer. FDG-PET is also used for evaluation of recurrent thyroid cancer, usually in the scenario where despite a rising thyroglobulin level, iodine-131 scan does not show activity. These iodine negative metastases are better detected with FDG-PET.10 FDG-PET is also useful for more aggressive biologically active tumors such as medullary and anaplastic cancers and remains useful for the detection of distant metastases.
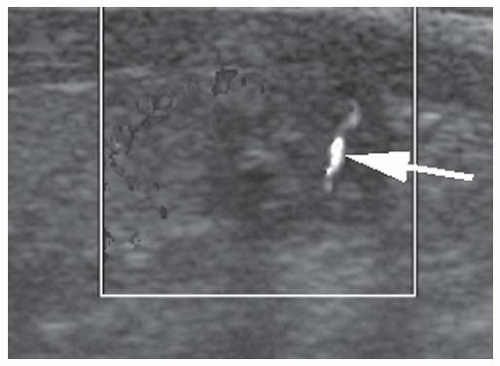 FIGURE 28-16. Ultrasound image of a thyroid nodule being biopsied with fine-needle aspiration. The needle is seen in the nodule as an echogenic line (arrow). |
Once the diagnosis of thyroid cancer is established, CT or MRI can be used for staging. CT is limited as intravenous iodinated contrast hinders subsequent postoperative tumor ablation or scanning with radioactive iodine for several weeks. MRI is therefore the study of choice. Both modalities can assess extension of tumor outside of the thyroid capsule (Fig. 28-17). The amount of extraglandular extension is important for surgical planning. MRI is best for imaging invasion of the trachea and esophagus. Axial T2-weighted images are especially useful for demonstrating invasion of the esophageal wall (Fig. 28-18). CT may be better at demonstrating invasion of the laryngeal cartilages (Fig. 28-19). Both CT and MRI can document encasement of the carotid artery (Fig. 28-20) or invasion of the jugular vein (Fig. 28-21), as well as involvement of the recurrent laryngeal nerve resulting in hoarseness.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


