Radiation Therapy Technique
William M. Mendenhall
The technique employed depends on the site and extent of the melanoma. The most common indication for radiotherapy (RT) in head and neck melanoma is for postoperative RT after resection of a lesion associated with a positive regional lymph node(s).1 A common site of lymph node metastasis is the parotid gland alone or combined with cervical lymph nodes. The parotid may be treated with an appositional electron field; the energy will depend on the depth-dose desired and is often 12-MeV electrons. If it is necessary to treat to 4 to 5 cm depth, higher-energy electrons may be “mixed” with 6 MV x-rays to reduce the skin dose. In this instance, the electron field is 1 cm larger than the x-ray field, except where it matches the low neck field, due to
beam constriction (Fig. 24-15). The anterior 6-MV x-ray field is matched with the parotid field(s) at the level of the thyroid notch. Alternatively, the parotid may be treated with intensitymodulated RT (IMRT).
beam constriction (Fig. 24-15). The anterior 6-MV x-ray field is matched with the parotid field(s) at the level of the thyroid notch. Alternatively, the parotid may be treated with intensitymodulated RT (IMRT).
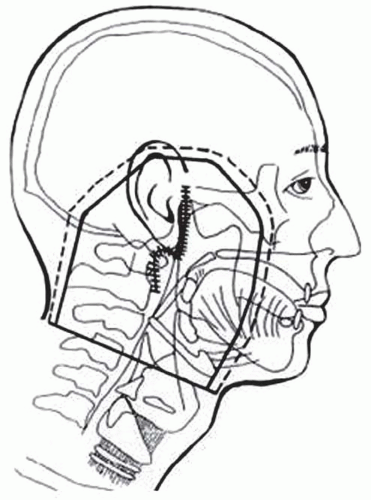 FIGURE 24-15. Appositional electron beam (dashed line) combined with 6-MV x-rays (solid line) to treat the parotid postoperatively. |
Posterior cervical lymph nodes may be treated with opposed photon fields and reduced off the spinal cord once cord tolerance has been reached and the anterior aspect of the neck over the spine treated with 10-MeV electrons to the desired dose.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


