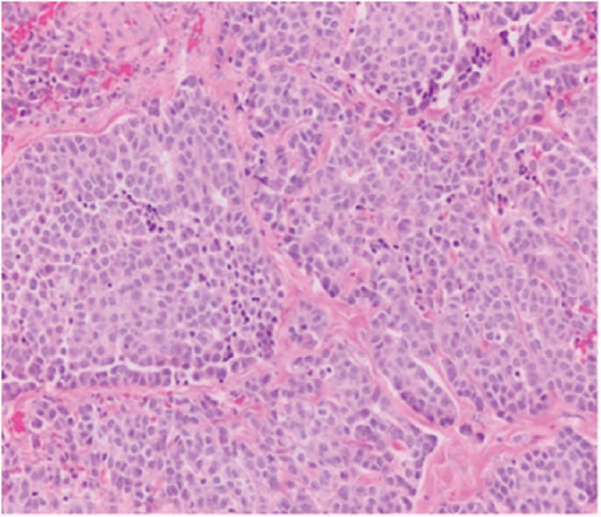
A 65-year-old white man with a past medical history of hypertension (HTN) and chronic obstructive pulmonary disease (COPD) presents with persistent cough for the last 4 months. A chest x-ray reveals a solitary lesion in the right middle lobe. Chest computed tomography (CT) confirms a 4-cm non-spiculated lesion without any associated lymphadenopathy. Endobronchial ultrasound-guided fine-needle aspiration biopsy reveals bronchial carcinoid with no evidence of necrosis or mitosis under a high-powered field (HPF). Learning Objectives: 1. What are the common presenting features of carcinoid? 2. What is the most sensitive and specific imaging study for carcinoid diagnosis? 3. What are the two characteristic microscopic features that differentiate typical and atypical carcinoid? 4. What is the first line of therapy for metastatic carcinoid? Carcinoids represent 1.2% of all primary lung malignancies. Their incidence in the United States has increased rapidly over the last 30 years and is currently about 6% per year.1 Typical carcinoids represent 80%-90% of all lung carcinoids and occur more frequently in the fifth and sixth decades of life. Nearly all bronchial neuroendocrine tumors (NETs) are sporadic; however, they can rarely occur in the setting of multiple endocrine neoplasia type 1 (MEN1). No external environmental toxin or other stimulus has been identified as a causative agent for the development of pulmonary carcinoid tumors. About 60% of the patients with bronchial carcinoid are symptomatic at presentation (Figure 22-1). The most common clinical findings are those associated with bronchial obstruction, such as persistent cough, hemoptysis, and recurrent or obstructive pneumonitis. Wheezing, chest pain, and dyspnea also may be noted. Although uncommon, various endocrine or neuroendocrine syndromes can be initial clinical manifestations of either typical or atypical pulmonary carcinoid tumors.2 Figure 22-1. Peripheral bronchial carcinoid. Chest radiography is abnormal in about 75% of patients with a pulmonary carcinoid tumor. A CT scan provides excellent resolution of tumor extent, location, and the presence or absence of mediastinal adenopathy. Because carcinoid tumors are highly vascular, they show greater enhancement than benign lesions on contrast CT. Although highly vascular, carcinoid tumors of the lung do not show increased metabolic activity on positron emission tomography (PET) and would be incorrectly designated as benign lesions on the basis of findings from a PET scan. The overexpression of somastatin receptor (SSTR) is a characteristic feature of bronchial NETs, which can be used to localize the primary tumor and its metastases by imaging with the radiolabeled somastatin (SST) analogues. Ga-DOTATATE/TOC scan also provides an estimate of receptor density and evidence of the functionality of receptors, which helps with selection of suitable treatments that act on these receptors. Serum levels of chromogranin A in bronchial NETs are expressed at a lower rate than other sites of carcinoid tumors. Hence, its measurement is of limited utility in following disease activity in bronchial NETs. For central tumors, transbronchial tumors, and peripheral tumors, CT-guided percutaneous biopsy is the accepted diagnostic approach. The diagnostic yield of brush cytology is low overall (4%-63%); hence, fine-needle biopsy is preferred. Distinction between typical and atypical carcinoid is made based on the presence of one or more of the following features (Figure 22-2, Table 22-1)3: Figure 22-2. Nests of lightly eosinophilic cells with relatively low nuclear grade and granular chromatin. TABLE 22-1 Distinguishing Features Between Typical Versus Atypical Carcinoid3
22
PULMONARY CARCINOID
CLINICAL PRESENTATION

Diagnostics
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


