Chapter 30 Primary Myelofibrosis
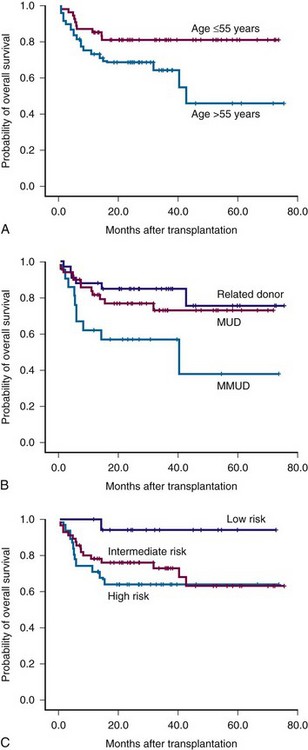
Figure 30-1 Survival of patients with myelofibrosis after reduced-intensity allogeneic stem cell transplantation according to age (A), donor (B), and Lille risk profile (C).
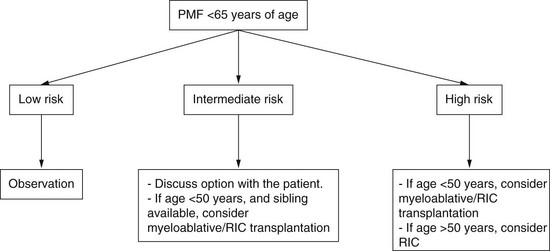
Algorithm for Selection of Appropriate Patients for Stem Cell Transplantation Stratified According to Risk Status