Key Points
- •
Cancer physical therapy is the evidence-based, reimbursed medical care used to specifically examine, assess, and treat impairments related to cancer and cancer treatment.
- •
Though physical therapy is readily available to patients, it remains underutilized in most cancer programs.
- •
If a cancer physical therapy program is focusing solely on patients with lymphedema or postoperative breast surgery, it is missing the vast majority of its potential volume and value.
- •
Evidence suggests cancer physical therapy may impact quality of life, length of survival, recurrence risk, and overall survival in patients with cancer.
- •
Cancer physical therapy demonstrates outcome benefits for cancer patients and for cancer programs.
- •
Physical therapy for patients with cancer should begin during the peri-diagnosis period and continue through survivorship.
- •
Physical therapy for patients with breast cancer should start with first cancer treatment intervention whether it be neoadjuvant chemotherapy or surgery.
- •
Cancer physical therapy is a low-cost, low-risk, nonpharmacological intervention that may decrease length of hospital stays, decrease hospital readmissions, decrease emergency department visits, and decrease fall risk.
- •
This chapter is solely focused on physical therapy for patients with breast cancer. However, impairments in patients with cancer result from surgery, chemotherapy, and radiation. Therefore, a rehabilitation consult should be offered to all patients undergoing cancer treatment, regardless of cancer type.
An Introduction to Breast Cancer Physical Therapy
Medical management for malignant breast disease includes surgery, chemotherapy, radiation, hormonal therapy, immunotherapy, and biological therapy. Each of these antineoplastic interventions has potential negative impacts on the human physiological, cardiopulmonary, integumentary, and musculoskeletal systems. As a result, well-established short-term, long-term, and late morbidities are often present in patients exposed to these cancer treatments. These morbidities, in turn, may result in decreased functional performance, loss of activities of daily living (ADLs) capacity, decreased quality of life, impaired sexual health, impaired social function, and loss of vocational, recreational, and exercise capacity. Evidence exists also, that this overall decrease in functional, physical, and physiological performance may negatively impact life span.
Though common, these symptoms often go under addressed, and though some physical and functional loss with cancer surgery, radiation, and cytotoxic and cytostatic treatments for breast cancer is expected, much of this loss is unnecessary and preventable. Evidence suggests physical therapy can prevent, minimize, or eliminate many of these cancer treatment-related symptoms and impairments.
Cancer rehabilitation is the medical modality used to specifically examine, assess, and treat the musculoskeletal, cardiopulmonary, physiological, integumentary, and functional impairments expected with cancer treatment, survivorship, advanced disease, and end of life. A vast body of quality studies show rehabilitation may increase quality of life, length of life, and that exercise may increase overall survival and decrease risk of recurrence in patients with breast cancer. Breast cancer rehabilitation services are provided by physical therapists, occupational therapists, and physiatrists. In the case of metastatic breast cancer (MBC) impacting a patient’s cognition, language, speech, breathing, or swallowing, a speech-language pathology consult may also be warranted.
Like other areas of specialization in physical therapy, such as orthopedics, neurology, geriatrics, etc., rehabilitation for patients with cancer is similarly evidence based and reimbursable. Physical therapists treat presenting impairments with the scientific application of therapeutic procedures with the goal of improving or preventing physical and physiological impairments and optimizing health and function. Skilled interventions used by rehabilitation therapists include, but are not limited to, therapeutic exercise, therapeutic activities, manual therapy, mechanical traction, ultrasound/phonophoresis, vasopneumatic devices, aquatic therapy, biofeedback, neuromuscular reeducation, orthotic/prosthetic use, cognitive performance testing, debridement, functional capacity evaluations, ADLs/self-care interventions, gait training, sensory integration, electrical stimulation, splinting/orthotics, prosthetic training, and wheelchair management. The most common of these interventions used in cancer rehabilitation include therapeutic exercise and manual therapy.
The National Accreditation Program for Breast Centers and the Commission on Cancer recognize the importance of cancer rehabilitation and have it as a required standard of a cancer care program. In its Optimal Resources for Cancer Care Guide, the Commission on Cancer states, “The availability of rehabilitation care services is an essential component of comprehensive cancer care, beginning at the time of diagnosis and being continuously available throughout treatment, surveillance, and, when applicable, through end of life.” The National Comprehensive Cancer Network (NCCN) also recognizes the benefits of rehabilitation and in its Guidelines for Cancer-Related Fatigue, it recommends referral to rehabilitation from diagnosis to end of life.
An Overview of Breast Cancer Physical Therapy
Traditionally, patients with breast cancer are referred to rehabilitation for postoperative and lymphedema-related care. Postoperative breast surgery symptoms and impairments amenable to rehabilitation include regional pain and swelling, weakness, limited shoulder range of motion (ROM), soft tissue shortening and soft tissue restrictions, cording, decreased ADL, vocational and recreational capacities, and risk for the development of lymphedema. Rehabilitation is effective in minimizing or eliminating this symptomology. However, if rehabilitation therapists and cancer practitioners focus solely on the postoperative symptoms and discontinue physical therapy when these problems are resolved, patients continuing with adjuvant treatment will not benefit from best practice care. Patients additionally undergoing chemotherapy, radiation, hormonal, and/or biological antineoplastic therapies will be exposed to additional potential symptoms and impairments from each of these individual cancer treatments.
Surgery, chemotherapy, radiation, hormonal therapies, and biological therapies may each result in unique musculoskeletal, cardiopulmonary, physiological, and integumentary impairments ( Table 11.1 ). Resultantly, symptoms and impairments amenable to rehabilitation will present at varying times throughout the cancer treatment continuum. To maximize best patient outcomes in breast cancer care, timely, seamless, evidence-based rehabilitation care across the cancer care continuum is recommended. The addition of rehabilitation therapists to the comprehensive oncology care team is pertinent for maximal patient health and outcomes during and after treatment for cancer.
| Medical Intervention/Disease Insult | Potential Resulting Physical/Physiological/Functional Impairments Amenable to Rehab | Outcome(s) Expected With Rehabilitation |
|---|---|---|
| Neoadjuvant chemotherapy | Fatigue, cardiotoxicity, weight gain, barriers to exercise, functional loss, decreased performance status/ADL capacity | Minimized fatigue, weakness, functional loss |
| Maximized performance status and cardiopulmonary function, minimized risk or amount of cardiotoxicity | ||
| SLNB (Sentinel lymph node biopsy) | Pain, limited arm/shoulder ROM, arm/shoulder weakness, cording, lymphedema risk, functional loss | Full preoperative pain-free mobility, strength, and function without limitation at involved upper quarter(s) |
| Minimized risk of lymphedema | ||
| ALND (axillary lymph node dissection) | Pain, limited arm/shoulder ROM, arm/shoulder weakness, cording, lymphedema risk, functional loss | Full preoperative pain-free mobility, strength, and function without limitation at involved upper quarter(s) |
| Minimized risk of lymphedema | ||
| Partial mastectomy | Pain, limited shoulder ROM, shoulder weakness, functional loss, expected pending radiation (see Acute Curative Radiation) | Full preoperative pain-free mobility, strength, and function without limitation at involved upper quarter(s) |
| Mastectomy | Pain, limited shoulder ROM, shoulder weakness, functional loss | Full preoperative pain-free mobility, strength, and function without limitation at involved upper quarter(s) |
| Breast reconstruction—tissue expander/implant | Pain, limited shoulder ROM, shoulder weakness, soft tissue tightness and restrictions, functional loss | Full preoperative pain-free mobility, strength, and function without limitation at involved upper quarter(s) |
| Breast reconstruction—tissue transfer | Pain, limited shoulder ROM, shoulder weakness, soft tissue tightness and restrictions, functional loss | Full preoperative pain-free mobility, strength, and function without limitation at involved upper quarter(s) |
| Cytotoxic chemotherapy | Fatigue, nausea, cardiotoxicity, weight gain, barriers to exercise | Minimized fatigue, weakness, functional loss |
| Maximized performance status and cardiopulmonary function | ||
| Bone marrow support drugs (pegfilgrastim) | Pain, barrier to function and exercise | Educated in bone flair and alternative activity and exercise options |
| Minimized functional loss | ||
| Acute curative radiation | Pain, fatigue, limited shoulder ROM and function, functional loss, barriers to full function and exercise | Minimized fatigue, weakness, functional loss |
| Maximized performance status and cardiopulmonary function | ||
| Post curative radiation | Soft tissue tightness and restrictions, risk for lymphedema, soft tissue pain, fatigue, weakness | Minimized fatigue, weakness, functional loss |
| Maximized performance status and cardiopulmonary function | ||
| Hormonal therapy (AI) | Arthralgias, myalgias, barriers to function and exercise | Good patient understanding of mechanism of arthralgia/myalgia |
| Patient educated in adapted exercise as needed | ||
| Patient compliant with 150 min/week exercise | ||
| Survivorship issues—long-term effects | Fatigue, pain, distress, barriers to full function and exercise | Independent in full body progressive resistive and aerobic exercise program Patient compliant with 150 min/week exercise |
| Survivorship issues—late effects | Lymphedema, cardiotoxicity-related dysfunctions, BMI change, CIPN, barriers to full function and exercise | Minimized lymphedema with maximized function |
| Patient compliant with 150 min/week exercise | ||
| Stage IV disease (months to years life expectancy) | Pain, muscle weakness, cardiopulmonary weakness, bone metastasis pain, fracture risk, limitations related to brain mets, distress, altered performance status | Maximized performance status, cardiopulmonary strength, bone health, compliance with 150 min/week exercise |
| End-stage disease (days to weeks life expectancy) | Pain, fall risk, unsafe transitional movements and balance, unsafe gait, altered performance status | Maximized ADL independence, safety, function, gait, quality of life |
| Minimized fall risk | ||
| Patient and family education in safe transfers and in home mobility and function | ||
| Patient and family educated in pain reduction positioning and techniques |
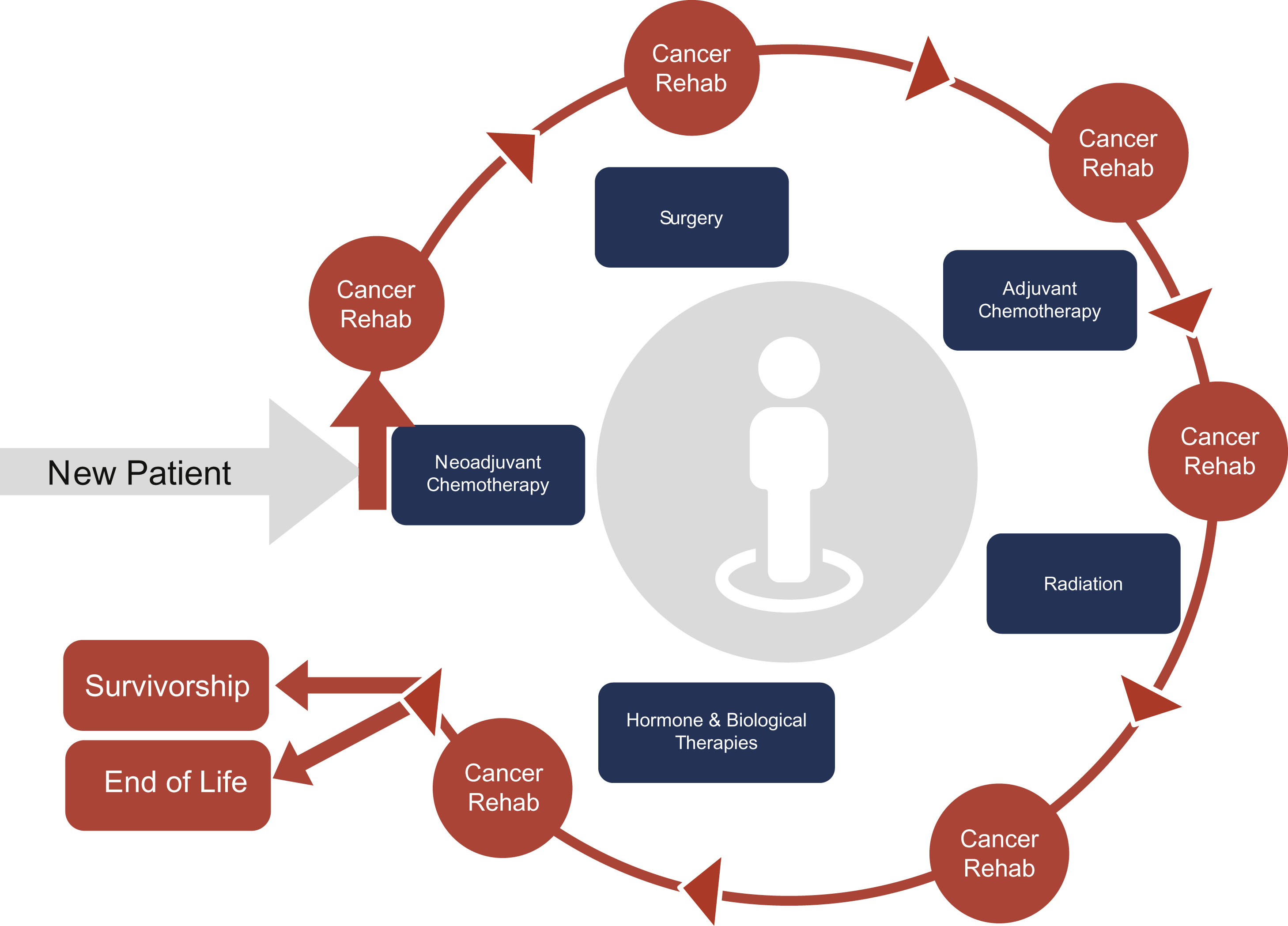
As a patient moves through medical treatments, cancer rehabilitation best practice involves the rehabilitation therapist providing active surveillance and rehabilitative treatment and education, based on the patient’s symptom profile and functional needs ( Fig. 11.1 ).
Impairments treated by oncology physical therapists include, but are not limited to, increased pain and symptoms, headaches, and impairments in posture, strength, ROM, scapulohumeral rhythm, muscle length and flexibility, tissue mobility, tissue and wound healing, joint mobility, gait, mobility, activity tolerance, balance, motor function/performance, coordination, sensory integration, body mechanics, bladder health, bowel health, and sexual health, as well as increased swelling and risk for falls.
Referring to Breast Cancer Physical Therapy
Oncology practitioners are encouraged to refer patients undergoing or pending cancer treatment to an oncology physical therapist in the peri-diagnosis period. Referrals from physicians, physician assistants, and nurse practitioners are generally third-party reimbursed. In some regional areas, payors and health systems may additionally offer direct access to physical therapists. If the patient is beginning breast cancer treatment with neoadjuvant chemotherapy, referral to oncology physical therapy should be made in the peri-diagnosis period, ideally prior to the onset of cycle one. If surgery is the patient’s first anticancer intervention, physical therapy should begin as soon as possible postoperatively at the breast or reconstructive surgeon’s discretion. If the patient is doing well postoperatively with pain control, is maintaining mobility and independence, and is on a walking program, physical therapy may begin as soon as possible after the drains are removed. If the patient does not have postoperative drains, is experiencing moderate to severe chest wall or axillary pain, has cording, or has less than 90 degrees of shoulder flexion/abduction with pending radiation, rehabilitation may begin at 1 to 2 weeks post breast surgery.
After a patient’s injury or illness involving cardiology, neurology, or orthopedics, early mobilization with physical therapy is commonplace. Though not routine in oncology, this principle of early mobilization is also warranted. For example, even with the presence of postoperative restrictions, early referral to physical therapy post surgery remains beneficial. In this time, education and training in walking or aerobic exercise within postsurgical limitation can begin. Additionally, instruction in ADL modifications and safe strength exercises for the legs and nonsurgically affected muscles of the upper body can begin. If the patient is experiencing moderate to severe pain from cording or soft tissue restrictions or shortening, manual therapy and therapeutic exercise may be effective within the lifting and ROM postsurgical restrictions. This early postoperative period also allows the rehabilitation therapist to identify patients awaiting radiation simulation and treatment planning who do not have adequate pain control or the ROM at both glenohumeral joints needed to tolerate this treatment. Alerting the radiation oncologist to this potential can decrease the risk of failure to complete the full simulation and planning which has financial impacts and is a dissatisfier for both the patient and the radiation oncology team.
Ultimately, these early postoperative interventions may decrease the need for narcotics and other pain medications, minimize cardiorespiratory depression, maintain functionality, promote independence, better prepare patients for return to work, decrease patient distress, and set the expectation of the benefit of being active throughout their entire cancer treatment regimen.
Breast Cancer Surgery: Implications for Physical Therapy
Section Key Points
- •
Postoperative breast cancer surgery physical therapy has shown to improve outcomes in both the short and long term and lowers the risk of long-term pain.
- •
Physical therapy presents patients with a high likelihood of regaining their preoperative ADLs, vocational, and social activities. Physical therapy does not increase the incidence of postoperative complications, including dehiscence, seroma, infection, or necrosis.
- •
Patients participating in postoperative physical therapy are less likely to overlimit themselves and preserve activity levels and strength, resulting in improved current and future treatment tolerability and outcomes.
- •
Postoperative breast cancer physical therapy does not increase adverse events, helps patients tolerate medical office visit burden, and is cost effective.
- •
Even patients without pain or limitation after surgery should be referred in the postoperative period to develop strategies and an exercise prescription for pending chemotherapy, radiation, and hormonal therapies.
Efficacy of Postoperative Breast Cancer Physical Therapy
Breast cancer procedures include biopsy, partial mastectomy, mastectomy, sentinel lymph node biopsy, axillary dissection, oncoplastic procedures, and breast reconstruction. Each of these surgical interventions is known to potentially result in ipsilateral breast, anterior chest wall, lateral chest wall, and/or axillary pain, soft tissue restrictions, soft tissue shortening, muscle weakness, limited shoulder ROM, edema, and cording ( Box 11.1 ).
- •
Pain at the anterior chest wall, lateral chest wall, and/or axilla
- •
Limited range of motion at the involved shoulder(s)
- •
Soft tissue restrictions and shortening
- •
Cording at the abdomen, axilla, upper arm, antecubitus, forearm, hand, and/or fingers
- •
Upper quarter muscle weakness
- •
Postoperative swelling
- •
Postural change
- •
Loss of activities of daily living, social, recreation, vocational, and exercise function
This postsurgical morbidity of upper quarter pain and loss of normal tissue or joint mobility may lead to patient difficulties with ADLs, including decrease in functional tolerance, vocational capacity, exercise tolerance, quality of life and satisfaction, along with difficulty managing pending chemotherapy or radiation and an overall increase in distress. It is important to note that, because breast cancer operations typically do not alter glenohumeral or tendon, ligament or muscle function, most patients should expect eventual return to full pain-free preoperative function without restriction with physical therapy. This can set the realistic expectation that return to full pain-free preoperative strength, function, mobility, and activity is achievable for most patients with physical therapy. This, when presented to patients, helps reduce the fear of disability, worry, and distress which often accompanies a new cancer diagnosis.
Physical therapy post breast surgery is known to limit or eliminate postoperative morbidities, impairments, and disabilities. Patients receiving a physical therapy consult and education with treatment as needed have less opioid use, better shoulder, and upper quarter ROM, full or maximal arm and shoulder strength, a quicker trajectory to recovery, less distress, and improved patient satisfaction. This improves both short- and long-term outcomes for patients. Having less pain and mobility restores full function and independence allowing patients to return to preoperative comfort and activity which positions them to tolerate upcoming local or systemic cancer treatments.
Referral to Postoperative Breast Cancer Physical Therapy
An operation is usually the first medical modality in breast cancer treatment, making it the most common entry point for physical therapy. It should be noted, though, that patients receiving neoadjuvant chemotherapy should receive a rehab consult peri-diagnosis to develop an exercise prescription to combat treatment-related fatigue and musculoskeletal, cardiopulmonary, and functional loss (see section “Efficacy of Physical Therapy During Chemotherapy”).
Unlike other types of cancers, evidence does not support preoperative physical therapy for breast cancer operations as physical therapy interventions do not impact postoperative pain or function or decrease the length of the postoperative hospital stay. Breast surgeons and plastic surgeons should encourage patients to remain active, walk regularly after diagnosis, and after surgery as allowed within their restrictions. Referral of a patient to physical therapy in the postoperative phase and the associated postoperative patient restrictions is at the discretion of the referring surgeon. The most common factor impacting initiation of physical therapy is the presence of postoperative drains. Typically, physical therapy may start when the patient’s drains are removed. If patients have postoperative drains yet are reporting moderate to severe chest wall pain, axillary pain, symptomatic cording or have active ROM less than 90 degrees at either shoulder with pending radiation, they should be referred to physical therapy after discussion with their surgeon. Studies suggest earlier intervention is ideal.
Early rehabilitation in the presence of postoperative limitations and drains can still address modifications for ADLs, including a walking or aerobic program with a progressive resistive exercise prescription for noninvolved muscles. This intervention may minimize unnecessary distress, pain, and loss of function and help prepare them for any pending adjuvant systemic or local treatment.
Goals of Postoperative Breast Surgery Physical Therapy
The goals of physical therapy for patients after breast cancer surgery encompass three primary intents: (1) to return the entire upper quarter(s) to full or maximized pain-free preoperative tissue mobility and length, shoulder ROM, strength, and overall function; (2) to educate the patient in potential long-term and late effects of cancer surgery and how to minimize those risks, watch for them, and initiate an action plan if noticed; and (3) to promote patient compliance in a basic combined aerobic and resistive exercise program for pending chemotherapy, radiation, or survivorship and to ensure the patient understands the positive impact of this regular exercise on their treatment tolerability, overall health, cancer recovery, and decreased cancer recurrence.
Post–Breast Cancer Surgery Physical Therapy Subjective History
After surgery for breast cancer, patients may or may not have postoperative pain or functional limitation but still may benefit from physical therapy. Scar tissue development over the next few months may create soft tissue shortening and restrictions, pain, and decreased shoulder ROM, which could be prevented with a chest wall and axillary stretch program. Patients receiving adjuvant chemotherapy and/or radiation may benefit from the development of a personalized exercise prescription to mitigate treatment-induced fatigue. Patients need to be educated about long-term effects, including lymphedema, and learn their role in preventing these sequelae. Exercise may improve quality of life post breast cancer and decrease the risk of breast cancer recurrence.
Once the referral to oncology physical therapy is received, the physical therapist may consult with the referring clinician, the multidisciplinary cancer team, and the cancer nurse navigator, as well as complete a pertinent chart review. At the initial physical therapy evaluation, the therapist will take a subjective history and complaints, examine the patient, do tests and measures, and evaluate the results. Using these results, a determination can be made if the patient needs physical therapy treatment, and if so, what type of treatment, how much, and on what timeline.
In a standard subjective physical therapy evaluation, information is obtained on the patient’s past medical history, living situation, home environment, work status, and social and recreational activities. They will be questioned about their evaluation-related complaints, concerns, pain level, physical and functional limitations, and other pertinent information that may be impactful to their rehabilitation and recovery. Attention should be directed at previous injuries or physical dysfunction in the involved upper quarter(s), primarily at the glenohumeral joint(s).
Information should also be gathered on the patient’s past, current, and any pending cancer treatment. It is also of great importance to learn the patient’s exercise literacy, history, experience, preferences, access to exercise equipment, modes of exercise, and safe places to exercise, as well as any co-morbidities potentially affecting exercise compliance and tolerance. Gathering clinical data with standardized outcome tools are also warranted. Though not specific to breast cancer, subjective outcome tools such as the Quick Disability of the Arm, Shoulder and Hand (DASH), Lower Extremity Functional Scale (LEFS), Timed Up and Go, and the 6-Minute Walk Test will provide functional information to help develop a comprehensive physical therapy plan of care.
Post–Breast Cancer Surgery Objective Examination
At the postoperative objective examination, the physical therapist will assess the involved upper quarter for wound/incision healing and for the presence of abnormal swelling or redness. Any abnormal finding or signs suggestive of potential abscess, infection, dehiscence, or blood clot warrant immediate notification of the referring surgeon.
Because breast cancer surgery involves removing soft tissues, ensuing postoperative tissue restrictions, tissue shortening, and scarring may present over the next few weeks to months. As such, physical therapists, in addition to assessing shoulder, neck, and elbow ROM, should also assess the soft tissues in the surgical area. This involves testing length and mobility of the skin, connective tissue, and muscle at the anterior chest wall, lateral chest wall, and axilla. If the patient had lymph node surgery, the objective examination should look for the presence of cording at the chest, axilla, arm, hand, and/or fingers. The postoperative physical therapy exam should also include strength and functional assessment of the ipsilateral chest wall, scapular, shoulder, and arm muscles.
Post–Breast Cancer Surgery Rehabilitation Assessment
After examination, the physical therapist can make an assessment. This should include the resulting clinical impression, differential impairment diagnosis, the patient’s problem list, the patient’s goals, and their goal potential or prognosis. If the patient is presenting with pain, the physical therapist should determine the pain source, if possible. Pain in the postoperative patient may be from postsurgical change, nerve, swelling, cording, soft tissue restrictions or shortening, chemotherapy, support drugs, orthopedic injury, or recurrence.
Post–Breast Cancer Surgery Physical Therapy Plan of Care, Interventions, and Treatment
Based on the initial evaluation of subjective and objective data and the assessment, a physical therapy treatment plan of care for the noted impairments and their resulting disabilities will be developed. For example, a postoperative patient may present with decreased ROM with the resulting disability of not being able to dress themselves independently or reach adequately for full ADLs function. With these findings, a stretching program can be developed to address the soft tissue tightness where the patient would be educated in compensatory ADL techniques to regain the ability to dress and reach.
After breast cancer surgery, treatment is directed to reverse and/or prevent any impairments and to optimize the patient’s overall health and function. The most common of these interventions include therapeutic exercise (CPT code 97110) and manual therapy (CPT code 97140). Therapeutic exercise involves instructing a patient in specific exercises to address weakness or loss of joint mobility due to disease or injury. Manual therapy includes techniques such as manipulation, soft tissue mobilization, or joint mobilization.
A physical therapy plan of care should include treating any upper quarter integumentary or musculoskeletal dysfunctions like muscle weakness, cording, edema, soft tissue restrictions, limited ROM, and resulting loss of function. All breast surgery rehabilitation plans of care should include a walking program and strengthening for the core, arms, and legs if adjuvant chemotherapy, radiation, or hormonal therapies are pending.
The rehabilitative treatment frequency and duration can be determined in collaboration with the treating therapist, referring provider, and the patient and will be based on the type and severity of clinical findings ( Fig. 11.2 ).