Peritoneal carcinomatosis, mesothelioma, and sarcomatosis are included in the group of diseases collectively referred to, in this chapter, as peritoneal metastases. Over the past three decades, there has emerged an increasing optimism concerning an individualized management plan for cancer dissemination within the abdomen and pelvis. The clinical problem was originally defined by several important clinical studies that established the natural history of peritoneal surface malignancy.1,2,3
Concomitant with these manuscripts that identified the dismal prognosis of patients with peritoneal metastases, isolated reports appeared concerning an emerging technology that described a new approach to management. This alternative treatment plan had two essential components. First, cytoreductive surgery (CRS) was used in an attempt to resect all visible implants within the abdomen and pelvis. Peritonectomy along with visceral resections was developed to surgically eradicate cancer on peritoneal surfaces.4 The second component was local-regional chemotherapy (intraperitoneal chemotherapy) used in the operating room or within the early postoperative period before adhesions develop. Chemotherapy used in the operating room with moderate heat has been referred to as hyperthermic intraperitoneal chemotherapy (HIPEC)5; chemotherapy used within the early postoperative period has been referred to as early postoperative intraperitoneal chemotherapy (EPIC).6 The chemotherapy is used in an attempt to eradicate free cancer cells and minute attached nodules that remain following surgery.7
The unique aspect of this new combination of treatments was the perioperative timing of the chemotherapy. Currently, the perioperative chemotherapy may be both intravenous and intraperitoneal, and may be administered in the operating room or in the early postoperative period. HIPEC now abbreviates the term hyperthermic perioperative chemotherapy and includes all perioperative chemotherapy regimens. It is not adjuvant chemotherapy and it is not neoadjuvant chemotherapy; it is chemotherapy used simultaneously with a major cytoreductive surgical procedure. Of course, all efforts to maintain benefits from systemic chemotherapy in patients with peritoneal metastases or mesothelioma must continue. Patients with peritoneal surface malignancy are required to be a focus of the multidisciplinary team (MDT).
NATURAL HISTORY STUDIES DOCUMENT THE IMPORTANCE OF LOCAL-REGIONAL PROGRESSION
A strong rationale for the emergence of CRS and HIPEC as a valid treatment option comes from natural history studies. In a proportion of patients, recurrence of the primary cancer isolated to the surfaces of the abdomen and pelvis is a reality. Primary or recurrent disease at the resection site and on peritoneal surfaces in the absence of hepatic metastases or systemic metastases does occur; these patients are appropriate for treatment by CRS and HIPEC. Isolated peritoneal surface progression of abdominal or pelvic malignancy is not unusual.8,9,10,11,12
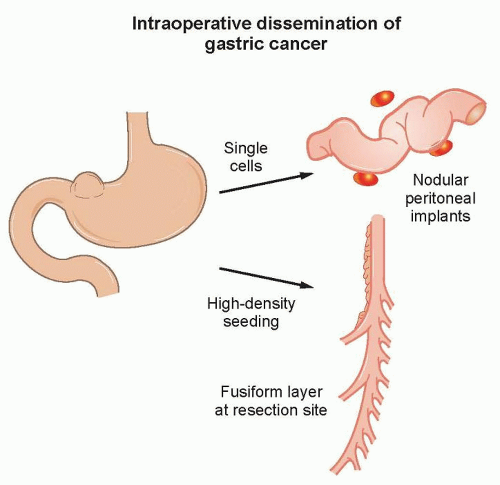
To fully understand the importance of cancer cells that gain access to the peritoneal space prior to or at the time of a cancer resection, one must appreciate the pathophysiology of disease. Figure 41.1 illustrates the mechanism of local-regional progression. Cancer cells at low density result in peritoneal metastases at a distance from the primary cancer resection. Cancer cells at higher density become trapped within raw tissue surfaces at the resection site. A fusiform layer of cancer that conforms to the anatomic structures within the bed of the primary resection site results from high-density seeding.13 The progression of cancer implants within the resection site and on peritoneal surfaces in the absence of liver metastases or systemic disease presents a major rationale for comprehensive local-regional treatments.14
PATIENT SELECTION USING QUANTITATIVE PROGNOSTIC INDICATORS
A second factor strongly recommending CRS and HIPEC as a valid treatment option comes from well-established selection factors applied to this patient population. With some variations between diseases, the same group of quantitative prognostic indicators operates for all patients with peritoneal surface malignancy. Now, prognostic indicators are used to refine the selection of patients to those most likely to benefit and to exclude those who are unlikely to benefit.15,16 Histopathology, the peritoneal cancer index (PCI), the completeness of cytoreduction score (CC), radiologic imaging by computed tomography (CT), and TNM (tumor, node, metastasis) stage with peritoneal cytology play a central role in patient selection.
Biologic Aggressiveness as Measured by Histopathology for Epithelial Appendiceal Neoplasms and Peritoneal Mesothelioma
Mucinous appendiceal neoplasms have a broad spectrum of aggressiveness, and the histologic type of the appendiceal neoplasm has a profound effect on survival following treatment by CRS and HIPEC.17 Patients with adenomucinosis obtain maximal survival benefit, while those with mucinous carcinoma show survivals similar to that for peritoneal metastases of colorectal origin.18
Seven different histologic patterns of peritoneal mesothelioma contribute to three distinct histologic groups that have a very different prognosis following treatment with CRS and HIPEC: poor prognosis for sarcomatoid, deciduoid, or biphasic types; intermediate prognosis for papillary and epithelial types; and excellent prognosis for low-grade or multicystic types.19,20
Figure 41.1 Intraoperative dissemination of gastric cancer cells. If cancer cells gain access to the peritoneal space either prior to or at the time of gastrectomy, two patterns of dissemination are observed. Low density of cancer cells into the free peritoneal space results in nodules as peritoneal implants. A high density of cancer cells dropped into the cancer resection site results in a layering of cancer.
Extent of Disease as Measured by the Peritoneal Cancer Index
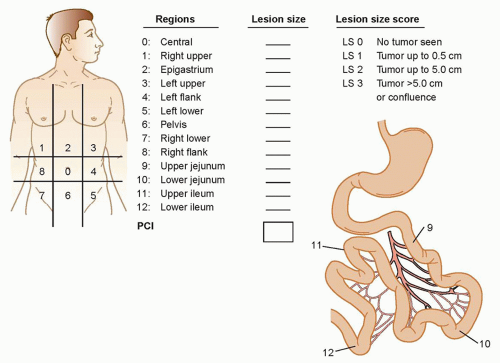
The PCI is an assessment combining lesion size (0 to 3) with tumor distribution (abdominopelvic regions 0 to 12) to estimate the extent of disease within the abdomen and pelvis as a numerical score (Fig. 41.2).21 It is calculated from observations obtained at the time of surgical exploration of the abdomen and pelvis, and should be recorded by the surgeon before leaving the operating room. The higher the PCI, the less likely CRS and HIPEC will result in longterm survival for all the peritoneal surface malignancies discussed in this chapter.
Figure 41.2 The peritoneal cancer index (PCI). This index combines a size and a distribution parameter to achieve a numerical score. The lesion size (LS) is used to quantitate the size of peritoneal nodules. The distribution of tumor is determined within the 13 abdominopelvic regions.
The Completeness of Cytoreduction Score Performed after the Resection
The size of residual tumor nodules visually determined after CRS has been completed has a profound effect on outcome. The new definition of complete cytoreduction is no visible evidence of cancer or only minute nodules reliably penetrated by HIPEC, a completeness of cytoreduction score of 0 (CC-0) or CC-1, respectively. With few exceptions, a CC-0 or CC-1 score is necessary for long-term benefit with CRS and HIPEC.21
Preoperative Radiologic Imaging by Computed Tomography
CT of the chest, abdomen, and pelvis is an essential tool in the selection of patients for CRS with HIPEC. Systemic metastases and spread to pleural surfaces can be identified. The location and quantity of mucinous carcinoma within the peritoneal cavity can be accurately determined.22,23 Unfortunately, nonmucinous peritoneal metastases may be greatly underestimated by CT.24 If the small bowel and its mesentery are layered by tumor or a large mass of cancer occupies the epigastric region, the likelihood of achieving complete cytoreduction is small. The CT should be performed with maximal intravenous and oral contrast in order to identify patients who have small bowel compartmentalization versus diffuse involvement of the small bowel and its mesentery.
Tumor, Node, Metastasis Stage, Peritoneal Cytology, and Clinical Features of the Primary Cancer
A careful survey of the peritoneal surfaces at the time of primary gastrointestinal cancer resection combined with a knowledgeable and timely gross and histopathologic assessment of the resected specimen can accurately predict the incidence of peritoneal metastases that will occur in follow-up. Also, in advanced gastrointestinal cancers, peritoneal cytology provides important prognostic information. This information should be used by the MDT to consider proactive treatment with CRS and HIPEC. It is possible to prevent peritoneal metastases in high-risk groups or treat peritoneal metastases by second-look surgery in patients with documented disease.25,26,27,28,29,30 The fast pace at which peritoneal metastases progress and the profound effect of extent of disease (PCI) on outcome indicate this approach. Table 41.1 presents the clinical features that should alert the MDT to a high risk for peritoneal metastases.31,32
Pharmacokinetic Advantage of Perioperative Chemotherapy
Another argument in favor of CRS and HIPEC as a treatment option for peritoneal surface malignancy is a well-studied pharmacologic rationale. As determined by physical properties, some chemotherapy agents are especially appropriate for hyperthermic use in the peritoneal cavity after CRS has been completed. Other cell cycle-specific chemotherapy agents are more appropriate for EPIC. As experience with different perioperative chemotherapy regimens has accumulated, the use of multipleagent chemotherapy given both intravenously and intraperitoneally has evolved and promises to be increasingly effective. Heat targeting of both intravenous and intraperitoneal chemotherapy to the peritoneal surface cancer nodule is a goal of treatment.
TABLE 41.1 Tumor, Node, Metastasis Stage, Peritoneal Cytology, and Clinical Features of the Primary Cancer as an Estimate of the Incidence of Subsequent Peritoneal Metastases to Guide Proactive Treatment Strategies
Clinical Feature
Incidence of Peritoneal Metastases Observed in Follow-up (%)
Colorectal Cancer
Gastric Cancer
Peritoneal nodules detected with primary cancer resection
aData from Honore C, Goere D, Souadka A, et al. Definition of patients presenting a high risk of developing peritoneal carcinomatosis after curative surgery for colorectal cancer: a systematic review. Ann Surg Oncol 2013;20:183-192.
bData from Tsujimoto H, Hiraki S, Sakamoto N, et al. Outcome after emergency surgery in patients with a free perforation caused by gastric cancer. Exp Ther Med 2010;1:199-203.
Combined Use of Cytoreductive Surgery and Perioperative Chemotherapy as a Standard of Care in Selected Patients
A final argument for use of CRS and HIPEC as a treatment option for peritoneal surface malignancy concerns the well-defined management parameters that are currently in practice at experienced treatment centers. A standardized cytoreductive surgical procedure involves visceral resections and peritonectomy procedures in an attempt to leave the abdomen visibly free of cancer. After the CRS is complete, tubes and drains are positioned to facilitate inflow and outflow of the chemotherapy solution. The chemotherapy solution circulates through roller pumps and a heat exchanger to maintain moderate hyperthermia (42°C/109°F) within the abdomen and pelvis. The skin edges are elevated on a self-retaining retractor (open method) or the skin closed (closed method) in order to create a reservoir for the hyperthermic chemotherapy solution.
The sequence of cancer resection, intraoperative chemotherapy washing, and then intestinal reconstruction may be important to optimize the destruction of small volumes of cancer cells and prevent tumor cell entrapment in adhesions, suture lines, and the abdominal incision. During the peritonectomy and visceral resections, large volumes of cancer are removed; however, residual cancer cells remain and must be eradicated.
A review of the important recent contributions to the literature that critically assesses the benefits of CRS and HIPEC in different disease states constitutes the remainder of this chapter.
APPENDICEAL MALIGNANCY
Natural History
Although similarities exist, there are unique features of appendiceal malignancies as compared to colorectal adenocarcinoma. The first and probably the most obvious difference between the colon and the appendix malignancies is the diameter of the bowel lumen involved. A colon tumor grows as an intraluminal mass in the bowel and will invade through the wall. The intraluminal growth pattern causes the primary cancer to reach the serosa in a late stage. In contrast, the appendix is a small organ, up to 1 cm in diameter, with a thin wall. A tumor may obliterate the appendix lumen in an early stage. This may cause a rupture of the wall of the appendix, allowing a spreading of tumor cells into the abdominal and pelvic cavity. Early in the natural history of the disease, these neoplastic cells implant with a high efficiency throughout the peritoneal cavity and progress as peritoneal metastases.33,34
Histologic Classification
The biology of appendiceal malignancies varies from simple mucinous adenoma to solid intestinal type adenocarcinoma. The histology of the peritoneal metastases from the primary tumor itself has a major influence on the outcome of the treatment by CRS and HIPEC. Ronnett et al.35 and Bruin et al.36 described three different types in their analyses of appendiceal malignancies. Metastases with >90% mucus, flat epithelial cells, no atypia, and no mitoses had a good prognosis despite a high PCI. At the other end of the spectrum, peritoneal metastases with much atypia, abundant mitoses, and <50% mucus has a prognosis similar to colorectal carcinomatosis and is referred to as peritoneal carcinoma.
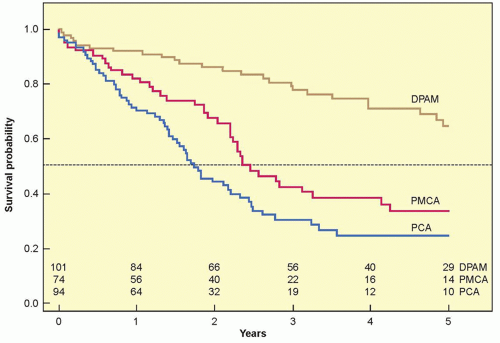
Figure 41.3 Survival of 269 patients with peritoneal metastases of an appendiceal neoplasm by histologic classification. DPAM, disseminated peritoneal adenomucinosis; PMCA, peritoneal mucinous carcinoma; PCA, peritoneal carcinoma. (From Bruin S, Verwaal VJ, Vincent A, et al. A clinicopathologic analysis of peritoneal metastases from colorectal and appendiceal origin. Ann Surg Oncol 2010;17:2330-2340.)
Outcome of Treatment of Peritoneal Dissemination by Cytoreductive Surgery Followed by Hyperthermic Perioperative Chemotherapy
The survival outcome with peritoneal dissemination of appendiceal origin neoplasms is shown in Figure 41.3. The overall survival is shown according to the histologic classification. For the least aggressive form (disseminated peritoneal adenomucinosis), the median survival is not reached within 5 years.36 Those patients who were affected by peritoneal carcinoma had a much poorer prognosis. The median survival was only 14 months in these patients. These survival data compare with the median survival of peritoneal metastases of colorectal origin treated with cytoreduction followed by HIPEC. Accepting the fact that complete resection is always the goal of CRS, these data document that survival with peritoneal metastases from appendiceal malignancies is highly dependent upon the histopathologic characteristics of the tumor.
Success in the treatment of recurrence after primary treatment with CRS followed by HIPEC is a unique feature of appendiceal peritoneal metastases. Benefit depends largely on the number and location of tumor masses. With a limited number of locations, the first choice is resection; if more diffuse disease is present and CRS is complete, a second HIPEC can be performed.37,38 In patients in whom the pathology is more aggressive, definitive treatment with systemic chemotherapy, with all it limitations, should be considered by the MDT.
Surgical Learning Curve
Cytoreduction followed by HIPEC is a complex treatment that demonstrates a surgical learning curve.39,40 The peak of the learning curve in the study of Smeenk et al.31 was reached after approximately 130 procedures. Surgical skill is undoubtedly the main component of this learning process, but modified treatment strategies for an individual patient and experience in handling complications by the entire medical team has contributed to a decreased morbidity and mortality.41,42
COLORECTAL PERITONEAL METASTASES: CURATIVE TREATMENT AND PREVENTION
Stage IV colorectal cancer is a very morbid disease, with a 5-year survival rate of 10% and a median survival of 14.4 months. The prognosis is significantly worse when peritoneal metastases are present, with a median survival of 6.7 months versus 18.1 months without peritoneal metastases (p <0.01).43 When colorectal peritoneal metastases are diagnosed, the crucial question for the MDT is whether curative (complete CRS with HIPEC) or palliative therapy (systemic chemotherapy) should be the goal of treatment.
Only gold members can continue reading. Log In or Register to continue