in breasts with cancer was compared with their prevalence in breasts without cancer (1). While these studies demonstrated that some benign lesions are more common in cancer-containing breasts, the histologic coexistence of certain benign breast lesions with breast cancer is not sufficient to establish that those benign lesions impart an increased cancer risk.
TABLE 9-1 Categorization of Benign Breast Lesions According to the Criteria of Dupont, Page, and Rogers (3) | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||
TABLE 9-2 Relative Risk of Breast Cancer According to Histologic Criteria of Benign Breast Disease in Four Studies Using the Criteria of Dupont, Page, and Rogers (3) | |||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||
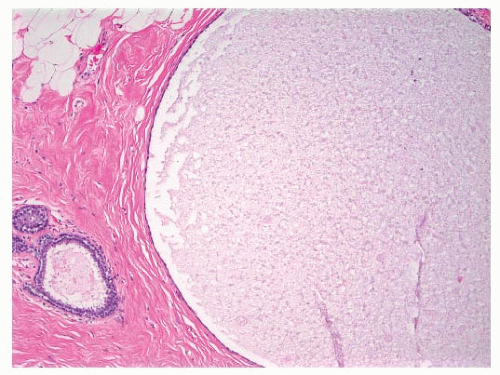 FIGURE 9-1 Cyst characterized by a large, dilated space filled with secretory material and lined by a flattened epithelial cell layer. |
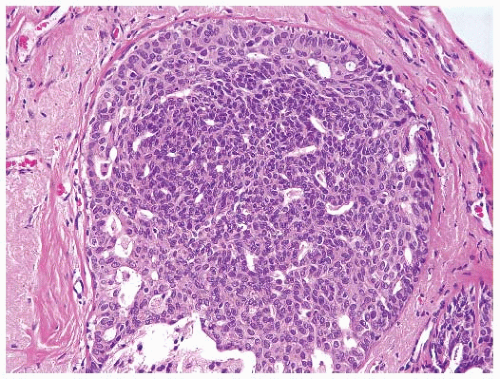 FIGURE 9-2 Usual ductal hyperplasia. A proliferation of cytologically benign epithelial cells fills and distends the duct. The nuclei vary in size, shape, and placement. The spaces within the duct are also variable in size and contour. |
or lobular type (3, 7). Atypical ductal hyperplasias (ADH) are lesions that have some of the architectural and cytologic features of low-grade DCIS, such as nuclear monomorphism, regular cell placement, and round regular spaces, in at least part of the involved space. The cells may form tufts, micropapillations, arcades, bridges, solid, and cribriform patterns (11). A second cell population with features similar to those seen in usual ductal hyperplasia is also typically present (Fig. 9-4).
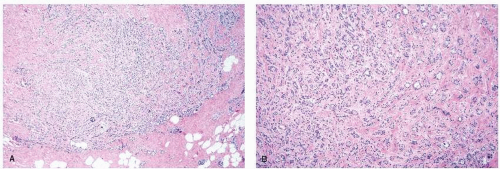 FIGURE 9-3 Sclerosing adenosis. (A) Low-power view demonstrates a lobulocentric proliferation of epithelial and stromal elements with scattered calcifications. (B) Higher-power view reveals glands and cords of epithelial cells entrapped in fibrotic stroma. The cells are cytologically benign, but the pattern simulates that of an invasive carcinoma. |
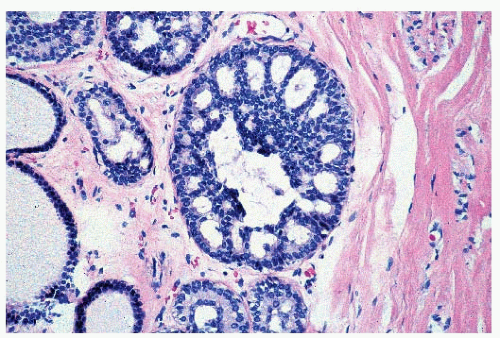 FIGURE 9-4 Atypical ductal hyperplasia. Near the center of this space is a proliferation of relatively uniform epithelial cells with monomorphic, round nuclei similar to those seen in low-grade ductal carcinoma in situ. However, these cells comprise only a portion of the proliferation within the space. |
not (16) (Table 9-3); at the present time this issue remains unresolved. Patients whose biopsies showed ALH involving both lobules and ducts had a higher relative risk of developing cancer (RR 6.8) than those with either ALH alone (RR 4.3) or those with only ductal involvement by atypical lobular hyperplasia (RR 2.1) (14).
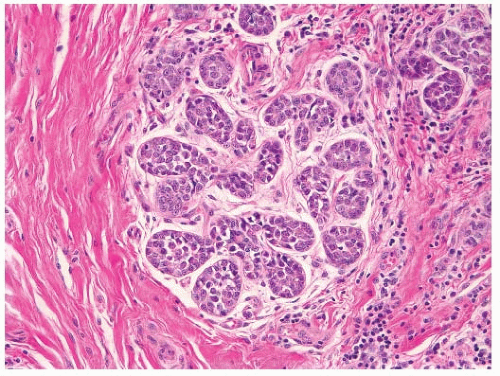 FIGURE 9-5 Atypical lobular hyperplasia. The acini of this lobule contain a proliferation of small uniform cells, which are dyshesive, and are identical to the cells that comprise lobular carcinoma in situ. However, the acini are not distended by this cellular proliferation. |
TABLE 9-3 Relative Risk of Breast Cancer According to Type of Atypical Hyperplasia | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
lesions without atypia who remained free of breast cancer for 10 years after their benign breast biopsy were at no greater breast cancer risk than women of similar age without such a history. In addition, the breast cancer risk among women with atypical hyperplasia was greatest in the first 10 years after the benign breast biopsy (RR 9.8) and fell to a relative risk of 3.6 after 10 years (18). In contrast, in an analysis of data from the Nurses’ Health Study, the breast cancer risk among women with proliferative lesions without atypia was similarly elevated before and after 10 years following the benign breast biopsy (RR 1.4 and 1.6, respectively). In addition, the risk associated with atypical hyperplasia was higher after 10 years (RR 5.2) than in the first 10 years after the benign breast biopsy (RR 3.3) (2). Similarly, in the Mayo Clinic study, an excess breast cancer risk was seen among women with biopsy-proven benign breast disease for at least 25 years after the benign breast biopsy (5). Among patients with atypical hyperplasia, the relative risk was persistently elevated beyond 15 years (16). More data are needed to clarify further the relationship between time since biopsy and breast cancer risk for women with benign breast disease, particularly for women with atypical hyperplasia.
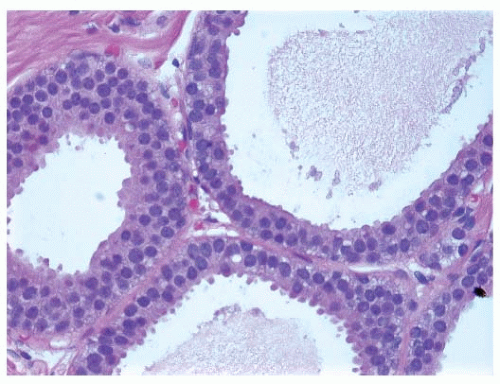 FIGURE 9-6 Flat epithelia atypia. The normal epithelial cells in the acini of this terminal duct are replaced by a population of columnar epithelial cells with round, monomorphic nuclei. |
TABLE 9-4 Effect of Family History of Breast Cancer on Relative Risk of Breast Cancer | |||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||
Related posts:
 Breast Cancer Screening
Breast Cancer Screening
 Ductal Carcinoma In Situ and Microinvasive Carcinoma
Ductal Carcinoma In Situ and Microinvasive Carcinoma
 Adjuvant Systemic Therapy: Endocrine Therapy
Adjuvant Systemic Therapy: Endocrine Therapy
 Preoperative Endocrine Therapy for Operable Breast Cancer
Management Summary for the Care of Patients with Metastatic Breast Cancer
Nursing Care in Patient Management and Quality of Life
Preoperative Endocrine Therapy for Operable Breast Cancer
Management Summary for the Care of Patients with Metastatic Breast Cancer
Nursing Care in Patient Management and Quality of Life
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


