22 Paediatric, teenage and young adult cancers
Introduction
In addition they have particular social, educational, developmental and psychological needs which, if not addressed, have long-term consequences for the patient and their family. Those who survive cancer at a young age may also be left with significant medical late effects which need to be recognized and managed (p. 58).
Incidence/epidemiology
The incidence of malignancy in the UK is:
Cancer is the most frequent natural cause of death in this age group, second only to accidents.
Types of cancer
The types of cancer vary not only between children and adults but as the age increases in certain age group bandings (Table 22.1).
Table 22.1 Distribution of cancer types according to age
| Age 0–14 years | Age 15–19 years | Age 20–24 years |
|---|---|---|
Clinical features
In children warning signs may be due to localized disease, or the manifestations of disseminated disease are listed in Box 22.1.
Box 22.1
Warning signs of cancer in children
Diagnosis and delays
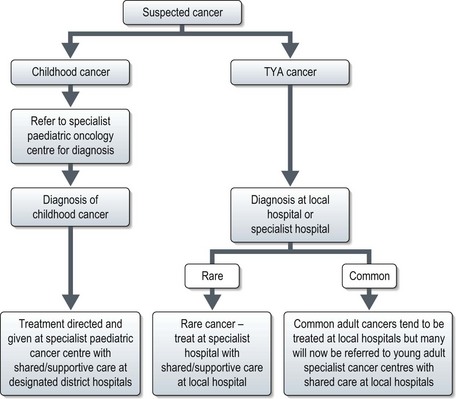
Diagnosis of malignancy currently follows the pathways for either paediatric or adult cancers. Paediatric cancers are diagnosed and treated in specialist principal treatment centres with some care shared with local hospitals. For TYA cancers, currently they may be seen in a paediatric or adult setting and treated according to those protocols. In the UK TYA cancer will soon be treated in specialized centres. This may mean referral to a specialist TYA centre or to an adult cancer specialist in a particular site of the body in a designated regional hospital with appropriate TYA facilities (Figure 22.1).
Specific childhood cancers
Leukaemias
In childhood acute lymphoblastic leukaemia (ALL) is by far the most frequently occurring leukaemia representing over 75% cases. (p. 308).
Presentation is usually with symptoms and signs of bone marrow infiltration and these can appear to occur quite rapidly, although are often preceded by several weeks of general malaise or recurrent infections and fevers. Usual features at the time of diagnosis are pallor, abnormal bruising or bleeding, bone pain (which may manifest as limping in young children) and on clinical examination lymphadenopathy and hepatomegaly in some children.
Diagnosis is suspected on the differential blood count but bone marrow examination is essential to confirm the diagnosis (p. 308), to perform immunocytochemical stains and cytogenetics which are of diagnostic and prognostic significance (Box 22.2).