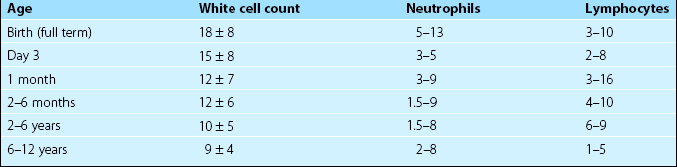
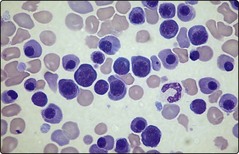
45 It is important to appreciate that the normal ranges for many haematological tests vary with age. Table 45.1 illustrates reference values for the total white cell count (WCC) and the differential count in children. More detailed listings of normal ranges of laboratory tests in childhood can be found in specialised paediatric haematology texts. Haemolytic disease of the newborn Severe HDN can result in intrauterine death. In the newborn child the presentation is entirely dependent on the degree of haemolysis but common features include anaemia, jaundice, oedema and hepatosplenomegaly. High levels of circulating unconjugated bilirubin may lead to high frequency deafness or deposition in the basal ganglia with spasticity and other neurological symptoms and signs (‘kernicterus’). Further investigation of the anaemia reveals features typical of haemolysis (Fig 45.1) with a positive direct antiglobulin test (DAT). In HDN due to RhD incompatibility the baby is RhD positive and the mother RhD negative with a high level of anti-D.
Paediatric haematology
Normal values
Neonatal disorders
Diagnosis
Paediatric haematology