Effective chelation therapy can prevent or reverse organ toxicity related to iron overload, yet cardiac complications and premature death continue to occur, largely related to difficulties with compliance in patients who receive parenteral therapy. The use of oral chelators may be able to overcome these difficulties and improve patient outcomes. A chelator’s efficacy at cardiac and liver iron removal and side-effect profile should be considered when tailoring individual chelation regimens. Broader options for chelation therapy, including possible combination therapy, should improve clinical efficacy and enhance patient care.
Transfusion-related iron overload
Regular red cell transfusions are used in the management of many hematologic disorders in children. In β-thalassemia major, transfusions relieve severe anemia, suppress compensatory bone marrow hyperplasia, and prolong survival. Regular red cell transfusions also are used frequently in children who have sickle cell disease, primarily to prevent and treat devastating complications, such as stroke. Other conditions that may be treated with transfusion therapy include Diamond-Blackfan anemia that is poorly responsive to steroids; Fanconi anemia; hemolytic anemias, such as pyruvate kinase deficiency; sideroblastic anemias; congenital dyserythropoietic anemias; and myelodysplastic syndromes.
In humans, iron is required for many essential functions, including oxygen transport, oxidative energy production, mitochondrial respiration, and DNA synthesis. Iron loss is limited to small amounts in the stool, urine, desquamated nail and skin cells, and menstrual losses in women, and humans lack physiologic mechanisms to excrete excess iron. Chronic red cell transfusion therapy leads to progressive iron accumulation in the absence of chelation therapy because the iron contained in the transfused red cells is not excreted efficiently.
Each milliliter of packed red cells contains approximately 1.1 mg of iron. A regular transfusion regimen usually consists of 10 to 15 mL/kg of packed red cells administered every 3 to 4 weeks to maintain a trough hemoglobin level of 9 to 10 g/dL in patients who have thalassemia and other congenital anemias and to maintain the hemoglobin S percentage at less than 30% in children who have sickle cell disease. This leads to an average iron accumulation of approximately 0.3 to 0.5 mg/kg per day, although there is considerable interpatient variability in iron loading. In addition, gastrointestinal iron absorption is increased greatly in patients who have ineffective erythropoiesis, such as thalassemia, and in some red cell enzyme deficiencies, in particular pyruvate kinase deficiency. The increased absorption of dietary iron can cause iron overload even in the absence of transfusions, although at a slower rate than that associated with chronic transfusions. Serial phlebotomy may be used to treat iron overload in some patients who have congenital anemia, but chelation therapy is needed to remove iron for those who have more severe anemia or transfusion dependence.
Hereditary hemochromatosis
Iron overload can result from hereditary causes that lead to increased intestinal absorption of dietary iron. Hepcidin, a small peptide produced by the liver in response to high iron levels and inflammation, inhibits iron absorption. Dysregulation of hepcidin now seems central in many of the hereditary forms of hemochromatosis. The most common form of hereditary hemochromatosis is caused by mutations in the HFE gene, which prevent the appropriate up-regulation of hepcidin expression in response to increased iron levels. A mutation causing a cysteine-to-tyrosine substitution (C282Y) in the HFE protein is common in those of Northern European ancestry and a second mutation causing a histidine-to-aspartic acid substitution (H63D) is distributed worldwide. Homozygosity for the C282Y mutation or compound heterozygosity for C282Y/H63D is associated with the development of iron overload, although clinical penetrance is variable. Clinical manifestations, including bronzing of the skin, cirrhosis, arthropathies, diabetes mellitus, and endocrinopathies, usually do not develop until middle age. Cardiac disease also can occur, although less commonly than with transfusional iron overload (discussed later). Mutations in the hepcidin gene or in another protein involved in hepcidin regulation, hemojuvelin, lead to a juvenile form of hemochromatosis with symptoms presenting by the third decade of life. The standard treatment for hereditary hemochromatosis is phlebotomy to reduce iron stores, although iron chelation therapy may be used in patients who are unable to tolerate the procedure.
Hereditary hemochromatosis
Iron overload can result from hereditary causes that lead to increased intestinal absorption of dietary iron. Hepcidin, a small peptide produced by the liver in response to high iron levels and inflammation, inhibits iron absorption. Dysregulation of hepcidin now seems central in many of the hereditary forms of hemochromatosis. The most common form of hereditary hemochromatosis is caused by mutations in the HFE gene, which prevent the appropriate up-regulation of hepcidin expression in response to increased iron levels. A mutation causing a cysteine-to-tyrosine substitution (C282Y) in the HFE protein is common in those of Northern European ancestry and a second mutation causing a histidine-to-aspartic acid substitution (H63D) is distributed worldwide. Homozygosity for the C282Y mutation or compound heterozygosity for C282Y/H63D is associated with the development of iron overload, although clinical penetrance is variable. Clinical manifestations, including bronzing of the skin, cirrhosis, arthropathies, diabetes mellitus, and endocrinopathies, usually do not develop until middle age. Cardiac disease also can occur, although less commonly than with transfusional iron overload (discussed later). Mutations in the hepcidin gene or in another protein involved in hepcidin regulation, hemojuvelin, lead to a juvenile form of hemochromatosis with symptoms presenting by the third decade of life. The standard treatment for hereditary hemochromatosis is phlebotomy to reduce iron stores, although iron chelation therapy may be used in patients who are unable to tolerate the procedure.
Organ toxicity related to iron overload
Free iron is toxic to cells and, therefore, iron normally is shielded by forming tight complexes with proteins. In plasma, iron is bound to transferrin, which transports iron to the cells. The main storage form of iron is ferritin, whereas hemosiderin is another iron storage protein, consisting of large iron-salt aggregates. Both are found principally in the liver, reticuloendothelial cells, and red cell precursors, but ferritin also is found in the blood, where it can be measured readily. In iron overload states, high levels of iron exceed the iron-carrying capacity of transferrin within the plasma, leading to accumulation of nontransferrin-bound iron. The nontransferrin-bound iron is taken up into cells, including liver, heart, and endocrine cells. Within the cells, the iron storage proteins become saturated, and instead, iron is bound only weakly to various low molecular weight proteins, known as labile iron. Iron that is not tightly bound can participate in the generation of free radicals that damage the cells leading to organ toxicity.
Most knowledge of the complications of iron overload comes from patients who have thalassemia who require lifelong red blood cell transfusions. Whether or not patients who have different diseases requiring chronic transfusions, in particular sickle cell disease, develop the same complications remains to be determined. Given the lack of substantial information about disease-specific responses to iron overload, data from the thalassemia population continue to guide monitoring and treatment for other transfused patient populations.
Iron overload leads to many clinical complications. Cardiac toxicity, including congestive heart failure and arrhythmias, is the leading cause of death related to iron overload in patients who have thalassemia major. Excess iron deposition in the liver leads to inflammation, fibrosis, and cirrhosis, which may be exacerbated by concomitant transfusion-acquired viral hepatitis. Iron is toxic to the endocrine organs, leading to growth failure, delayed puberty, diabetes mellitus, hypothyroidism, and hypoparathyroidism. In a report of 342 North American patients who had thalassemia major, 38% of subjects had at least one endocrinopathy, most commonly hypogonadism, and 13% had more than one endocrinopathy. Moreover, in that study, the prevalence of endocrine abnormalities increased with age, likely reflecting an accumulating iron burden. The goal of chelation therapy is to maintain the body iron at levels low enough to prevent the development of these organ toxicities. Once organ toxicity has developed, chelation therapy can reverse some of the complications, such as the cardiac complications (discussed later), although the endocrinopathies usually are not reversible.
Measurement of iron levels
There are several methods of assessing the degree of iron overload and each method has benefits and limitations ( Table 1 ). Thus, combinations of measurements, including serial measurements, are used in clinical practice to determine individual iron burden and response to iron chelation therapy over time.
| Method | Advantages | Disadvantages |
|---|---|---|
| Serum ferritin |
|
|
| Liver iron concentration by biopsy |
|
|
| Liver iron concentration by SQUID |
|
|
| Liver iron concentration by MRI |
|
|
| Cardiac iron loading by MRI |
|
|
The serum ferritin level is the test that is available most widely and easiest to perform. Because it is a simple blood test, many measurements can be performed without difficulty to establish trends in iron burden over time. In transfusional iron overload, the ferritin level correlates with total body iron burden, although the correlation is not precise, especially at higher values. Changes in the serum ferritin level in response to chelation have been shown to parallel changes in liver iron concentration measured by liver biopsy and noninvasive means. Thus, trends in serum ferritin levels may be useful for monitoring adequacy of chelation therapy. In addition, the ferritin level has prognostic significance for patients who have thalassemia major receiving chelation therapy with deferoxamine. Sustained levels of over 2500 μg/L are associated with an increased risk for organ toxicity and death. Thus, optimal chelation regimens should maintain the ferritin level at least lower than this value.
A limitation of the ferritin level is that a variety of disease states, including infection, inflammation, and ascorbate deficiency, can raise or lower serum ferritin levels. The limitation of ferritin in predicting iron stores is relevant particularly for patients who have sickle cell disease. In an analysis of 50 children who had sickle cell disease and were receiving regular red cell transfusions for primary stroke prevention in the Stroke Prevention Trial in Sickle Cell Anemia (STOP), great variability in the rate of rise of serum ferritin despite similar transfusion regimens was found among patients. Serum ferritin levels also underestimate liver iron concentration in patients who have thalassemia-intermedia and nontransfusion-associated iron overload.
Given that the liver is the major target organ for iron accumulation after multiple transfusions, the liver iron concentration is a good indicator of total iron burden. Various methods are available to estimate liver iron concentration, but liver biopsy generally is considered the gold standard for accurate iron measurement. In addition, this procedure allows direct assessment of liver inflammation and fibrosis. Liver iron concentration is a useful predictor of prognosis in patients who have thalassemia: levels in excess of 15 mg/g dry weight are associated with an increased risk for cardiac complications and death. Maintenance of the liver iron concentration between 3 and 7 mg/g dry weight in those receiving chelation therapy is considered ideal. Several limitations to liver biopsy exist, however. First, it is an invasive procedure, which restricts the acceptability to patients and its frequent use to monitor trends over time. In addition, liver fibrosis and cirrhosis cause an uneven distribution of iron, which may lead to an underestimation of liver iron in patients who have advanced liver disease. Finally, although high levels of liver iron predict an increased risk for cardiac disease, the converse not always is true: low levels do not always predict a low risk for cardiac disease. This may reflect the different organ-specific rates of iron accumulation and iron removal in response to chelation therapy. In patients who have a history of poor chelation and high iron levels in the past who subsequently use chelation, hepatic iron may be removed more rapidly then cardiac iron, so liver iron levels can fall before cardiac iron levels improve.
The superconducting quantum interference device (SQUID) technique uses magnetometers to measure very small magnetic fields and can be used as a noninvasive technique to measure ferritin and hemosiderin in the liver. Estimation of liver iron concentration by SQUID correlates linearly with concentrations measured by liver biopsy. Because this is a noninvasive technique, repetitive iron concentration measurements by SQUID have been used to monitor the efficacy of chelation in several studies. A major limitation to using SQUID is that it is a highly specialized and expensive approach. In addition, in recent clinical trials of the oral chelator, deferasirox, SQUID measurements underestimated liver iron concentrations obtained by biopsy by approximately 50%. Currently, only four sites worldwide offer the technology, limiting accessibility to patients.
MRI increasingly is used to monitor iron overload. This technique takes advantage of local inhomogeneities of the magnetic field caused by iron deposition in tissues. Magnetic resonance scanners are more widely available than SQUID, which should allow greater accessibility to patients. Differences in the type of machine, the strength of the magnetic field, and the analytic measurements, however, can limit accuracy and comparability among different sites. Although MRI may be used to estimate iron levels in a variety of organs, including the pituitary, pancreas, and bone marrow, it is used most commonly to measure hepatic and cardiac iron. MRI images darken at a rate proportional to the iron concentration. The darkening can be measured by two different techniques, spin-echo imaging and gradient-echo imaging. T2 refers to the time constant (half-life) of darkening for spin echo and T2 ∗ for gradient echo, with values inversely proportional to the amount of iron accumulation. The reciprocals of T2 and T2 ∗ , known as R2 and R2 ∗ , respectively, refer to rates of signal decay and are directly proportional to iron concentration. Studies using R2 to estimate liver iron show good correlation with iron levels determined by liver biopsy and reproducibility across different scanners. Other approaches using T2 ∗ or R2 ∗ also are promising for determining liver iron content. Cardiac iron levels also can be assessed using MRI, most commonly with T2 ∗ measurements. Determination of cardiac iron may be of greater clinical relevance than liver iron measurements because cardiac disease is the leading cause of death in patients who have thalassemia and transfusional iron overload. Cardiac T2 ∗ values below 20 ms indicate cardiac iron overload, whereas levels below 10 ms are associated with an increased risk for cardiac disease, including ventricular dysfunction and arrhythmias. Thus, patients who have very low cardiac T2 ∗ values may benefit from intensification of chelation therapy.
History of iron chelation
Deferoxamine, a naturally occurring iron chelator produced by Streptomyces pilosus , was the first iron chelator approved for human use. It is a hexadentate iron chelator that binds iron stably in a 1:1 ratio ( Table 2 ) . Deferoxamine is absorbed poorly from the gastrointestinal tract and has an extremely short half-life. Thus, it must be administered parenterally, usually as a continuous subcutaneous infusion (25 to 50 mg/kg given over 8 to 12 hours, 5 to 7 days per week). Iron bound to deferoxamine is excreted in urine and feces.
| Property | Deferoxamine | Deferiprone | Deferasirox |
|---|---|---|---|
| Chelator:iron binding | 1:1 | 3:1 | 2:1 |
| Route of administration | Subcutaneous or intravenous | Oral | Oral |
| Usual dosage | 25–50 mg/kg per day | 75 mg/kg per day | 20–30 mg/kg per day |
| Schedule | Administered over 8–24 hours, 5–7 days per week | Three times a day | Daily |
| Primary route(s) of excretion | Urine/feces | Urine | Feces |
| Adverse effects |
|
|
|
| Advantages | Long-term data available | May be superior in removal of cardiac iron | The only oral chelator licensed for use in United States |
| Disadvantages | Compliance problems may be greater |
|
|
| Special monitoring considerations |
| Weekly complete blood count with differential | Monthly blood urea nitrogen, creatinine, hepatic transaminases, and urinalysis |
The efficacy of deferoxamine is well established. In the 1960s, the ability of deferoxamine to induce substantial iron excretion and a net negative iron balance was demonstrated. Subsequently, in the 1970s, deferoxamine therapy was shown to reduce hepatic iron content and prevent progression of fibrosis. Most importantly, the use of deferoxamine is associated with a reduced incidence of cardiac complications and death. In addition, cardiac disease secondary to iron overload can be reversed with the use of deferoxamine, typically administered as a 24-hour infusion. Chelation therapy with deferoxamine prevents other organ toxicities, such as diabetes.
Local infusion site reactions, including induration and erythema, commonly are seen with administration of deferoxamine. Low zinc levels also can develop with deferoxamine use. Other adverse effects, including high frequency hearing loss, ophthalmologic toxicity, growth retardation, and skeletal changes, including rickets-like lesions and genu valgum, are more common when patients receive high doses of deferoxamine relative to their total body iron burden and can be minimized by maintaining an optimal chelator dose. Acute pulmonary toxicity with respiratory distress and hypoxemia and a diffuse interstitial pattern on chest roentgenogram is reported with the administration of high doses of deferoxamine (10 to 20 mg/kg per hour).
The major limitation to deferoxamine is the need to administer the drug parenterally, which is painful and time consuming. As a result, poor compliance remains a significant problem with administration of this drug, and preventable, premature deaths related to iron overload continue to occur.
Characteristics of an ideal chelator
The limitations of treatment with deferoxamine have led investigators to search for more acceptable iron chelators to be used in the management of iron overload. An optimal chelator should have adequate gastrointestinal absorption to allow oral administration, a long half-life permitting once or twice daily dosing, and a high affinity for iron with lesser affinities for other metals. The chelator should be able to induce iron excretion at a rate of at least 0.5 mg/kg per day to offset the amount of transfusional iron loading, and should be able to remove excess cardiac iron. Finally, toxicities associated with the drug should be minimal and manageable.
Deferiprone
Pharmacology
Deferiprone, or 1,2 dimethyl-3-hydroxypyrid-4-1 (Ferriprox), was the first orally active chelator studied extensively for the treatment of transfusional iron overload, introduced into clinical trials 20 years ago (see Table 2 ). Most studies have been open-label, noncomparative studies, often including patients who had a history of inadequate iron chelation, but a few randomized trials comparing deferiprone to deferoxamine are reported. A substantial amount of data on the safety and efficacy of the drug has been acquired, but considerable controversy surrounding the drug exists. In the European Union, deferiprone is approved for use for patients in whom deferoxamine therapy is contraindicated or inadequate, but the drug is not approved for use in North America and currently is available only to a limited number of patients through expanded access programs or research trials.
Deferiprone is a bidentate chelator, which forms a 3:1 chelator:iron complex. Given its short plasma half-life of 1.5 to 2.5 hours, the drug usually is dosed 3 times daily, although regimens of 2 or 4 times daily have been explored. The usual daily dose is 75 mg/kg per day, but higher doses have been studied. Deferiprone induces iron excretion almost exclusively in the urine, with minimal contribution from fecal elimination.
Efficacy
Urinary iron excretion with deferiprone at 75 mg/kg is comparable to that induced by deferoxamine at a dose of 50 mg/kg. Given that deferoxamine induces fecal iron excretion, total iron excretion with deferiprone is approximately 60% of that with deferoxamine at these doses. The mean urinary iron excretion with deferiprone at 75 mg/kg was 0.48 mg/kg per day in one study, a level predicted to maintain or decrease iron stores in most patients. Significant interpatient variability exists, however, so not all patients can achieve a negative iron balance at this dose. For example, in one study, urinary iron excretion ranged from 11.2 to 74.9 mg per day at a 75 mg/kg dosing level. Higher doses of deferiprone, 90 to 119 mg/kg, induced greater urinary iron excretion and may be beneficial for patients who have inadequate responses at lower doses.
Short-term studies of deferiprone generally show a reduction or stabilization in serum ferritin levels over a treatment period of 1 year or less. Similarly, studies that assessed the response to deferiprone over longer treatment periods, of 3 to 4 years, show reduced or stable mean serum ferritin levels. Similar responses are shown across different disease states, including sickle cell disease and thalassemia.
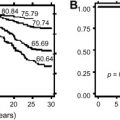
A small proportion of patients demonstrated a significant increase in serum ferritin levels while receiving long-term deferiprone. In a group of 151 Italian patients who received deferiprone for 3 years or more, 20% of subjects had clinically significant rises in ferritin levels during the first year of treatment. In general, patients who had higher baseline ferritin levels showed a greater reduction in serum ferritin than those who had lower pretreatment ferritin levels. In a long-term, multicenter study, 84 patients received deferiprone for 4 years at a mean daily dosage of 73 mg/kg. Mean serum ferritin levels declined significantly from 3661 to 2630 μg/L in the group whose baseline serum ferritin was above 2500 μg/L, whereas ferritin levels remained stable in those with baseline values less than 2500 μg/L.
Studies on the effect of chelation with deferiprone on liver iron content have mixed results. In a report of 21 patients who received deferiprone (75 mg/kg per day), mean liver iron concentration assessed by biopsy or SQUID decreased from 15 to 8.7 mg/g dry weight after an average of 3.1 years of treatment. Eight of 10 patients who had initial liver iron concentrations associated with a high risk for cardiotoxicity (>15 mg/g dry weight) had levels that fell to below that threshold with deferiprone treatment, and no patient who had lower initial hepatic iron concentrations rose above this threshold. With longer follow-up of a mean of 4.6 years in 18 patients, although there was an overall reduction in liver iron concentration from baseline (16.5 to 12.1 mg/g dry weight, P = .07), in seven patients, the liver iron concentration remained above 15 mg/g liver dry weight. In another report of 20 patients who received deferiprone (70 mg/kg daily) for 1 year or more, the mean liver iron content increased from 16 to 21 mg/g dry weight, although this change did not reach statistical significance. Liver iron content decreased in seven patients, rose in 12 patients, and remained the same in one patient. Thus, the data suggest that chelation with deferiprone (at a dose of 75 mg/kg per day) does not reduce liver iron concentration effectively in some patients.
Few randomized clinical trials have compared the efficacy of deferiprone directly to deferoxamine for the treatment of iron overload. In one study of 144 patients randomized to receive deferiprone (75 mg/kg per day) or deferoxamine (50 mg/kg per day), the reduction in serum ferritin levels after 1 year was similar between the two treatment groups. In a subset of 36 patients who underwent liver biopsy at the beginning and end of treatment, the mean reduction in liver iron content also was not significantly different between the two groups. In a more recent study, 61 Italian and Greek patients were randomized to receive deferoxamine (50 mg/kg daily for 5 days a week) or deferiprone (75 mg/kg per day initially, increasing to 100 mg/kg per day). The changes over a 1-year period in serum ferritin level and liver iron content assessed by SQUID did not differ significantly between the two treatment groups. In contrast, in a third study, in which 30 children were randomized into three groups to receive deferoxamine (40 mg/kg per day, 5 days per week), deferiprone (75 mg/kg daily), or combination treatment with deferiprone (75 mg/kg daily) and deferoxamine (40 mg/kg per day, twice weekly), after 6 months of treatment, those receiving deferoxamine alone had a significant reduction in serum ferritin, whereas the other two groups had a slight rise in ferritin levels.
The lack of reduction in serum ferritin or liver iron concentration in some patients receiving deferiprone may be explained by a variety of reasons, including poor compliance, variability in drug metabolism rate, or higher transfusional iron burden. The latter two problems potentially might be overcome by treating with a higher dosage of deferiprone. In one study, increasing the daily dose of deferiprone (from 75 mg/kg to 83 to 100 mg/kg) resulted in a fall in serum ferritin level in nine patients who had had inadequate chelation at the lower dose. Although no significant increased toxicity has been found in small studies using higher doses of deferiprone (up to 100 mg/kg daily), larger studies are needed to determine the long-term safety and efficacy of doses greater than 75 mg/kg per day.
Cardiac Iron Removal
A growing body of evidence supports the theory that deferiprone may be more effective than deferoxamine at removing iron from the heart and reducing iron-related cardiotoxicity. In one retrospective study, cardiac T2 ∗ and cardiac function were compared between 15 patients who had thalassemia and were receiving long-term deferiprone and 30 matched controls receiving long-term deferoxamine. Patients receiving deferiprone had significantly less cardiac iron (median T2 ∗ 34 ms versus 11.4 ms, P = .02). Furthermore, T2 ∗ values less than 20 ms, a level associated with excess cardiac iron, were found in only 27% of patients receiving deferiprone compared with 67% of those receiving deferoxamine ( P = .025), despite a significantly greater liver iron concentration in those receiving deferiprone. Left ventricular ejection fraction also was significantly higher in the deferiprone-treated group. Moreover, in a multicenter, retrospective study of patients who had thalassemia major, the risk for cardiac complications (cardiac failure or arrhythmia requiring drug treatment) was compared between 359 subjects who received only deferoxamine and 157 patients who received deferiprone. Fifty-two patients (14.5%) developed cardiac events, including 10 deaths from cardiac causes, during therapy with deferoxamine whereas no patients developed cardiac events during treatment with deferiprone or within 18 months of discontinuing therapy.
A few prospective trials have compared the effect of deferiprone to deferoxamine on cardiac iron removal and cardiac function. Two studies comparing deferiprone (75 mg/kg per day) to deferoxamine (50 mg/kg per day, 5–6 days per week) showed no significant difference in the reduction in cardiac iron between treatment groups after 1 year of therapy. A third study using similar dosing, however, showed a significantly greater reduction in cardiac iron and improvement in left ventricular ejection fraction with deferiprone than with deferoxamine after 3 years of therapy.
More recently, a multicenter, randomized, controlled clinical trial compared deferiprone (average dose 92 mg/kg per day) to deferoxamine (average dose 35 mg/kg per day, 7 days a week) for the treatment of 61 patients who had thalassemia major and abnormal cardiac T2 ∗ (<20 ms). Patients who had severe cardiac iron loading, T2 ∗ values less than 8 ms, or left ventricular ejection fraction less than 56% were excluded. A significantly greater improvement in T2 ∗ values was seen with deferiprone compared with deferoxamine after 1 year of treatment (27% versus 13%, P = .023). Similarly, left ventricular ejection fraction increased more in those treated with deferiprone (3.1% versus 0.3%, P = .003).
Adverse Effects
The most serious adverse event associated with deferiprone is agranulocytosis. In a multicenter study of 187 patients who had thalassemia major treated with deferiprone in which weekly blood counts were monitored, the incidence of agranulocytosis (absolute neutrophil count <500 × 10 9 /L) was 0.6 per 100 patient-years and the incidence of milder neutropenia (absolute neutrophil count 500 to 1500 × 10 9 /L) was 5.4 per 100 patient-years. In the largest study reported to date, similar rates for agranulocytosis (0.4 per 100 patient years) and for neutropenia (2.1 per 100 patient years) were reported. Neutropenia usually is reversible with discontinuation of the drug but often recurs with reinstitution of therapy. In clinical practice, blood counts should be obtained at least weekly and with all febrile illnesses or significant infections to monitor for this potentially life-threatening side effect. Treatment with deferiprone may not be appropriate for patients who have underlying bone marrow failure syndromes, such as Diamond-Blackfan anemia, who may be more likely to develop agranulocytosis or neutropenia. Similarly, caution should be exercised when using this drug in combination with hydroxyurea, interferon, or other drugs that can cause neutropenia.
Gastrointestinal symptoms, including nausea, vomiting, diarrhea, and abdominal pain, are common side effects reported with deferiprone, occurring in 33% of subjects in one large study. These symptoms usually occur in the first few weeks of treatment and rarely require discontinuation of therapy. Arthropathy with pain or swelling of the knees and other large joints is another common complication and can occur early or late in treatment. In a large study of 532 patients, the prevalence of this complication was only 4%, but other studies have reported higher rates of up to 38.5%. The arthropathy usually is reversible with discontinuation of the drug. Low plasma zinc levels developed in a minority of patients receiving deferiprone; thus, periodic monitoring of zinc levels is warranted.
Elevations in serum alanine aminotransferase (ALT) levels are observed in patients receiving deferiprone. This abnormality often is transient and resolves even if the drug continues to be administered at the same or reduced dose. Patients who have a higher iron burden and those who have hepatitis C infection may be more likely to develop ALT elevations. In addition, concerns have been raised regarding a possible progression of hepatic fibrosis with deferiprone therapy. In a retrospective study, five of 14 patients receiving deferiprone developed progression of liver fibrosis compared with none of 12 patients receiving deferoxamine. Four of the five patients who had worsening liver fibrosis also had antibodies to hepatitis C compared with only two of the nine subjects who did not have progression. In addition, the patients receiving deferiprone had higher baseline hepatic iron concentrations than the group receiving deferoxamine. Given that chronic viral hepatitis and iron overload may result in liver fibrosis, it is difficult to assess the contribution of deferiprone to progression of fibrosis. Other studies fail to show significant hepatic fibrosis attributable to deferiprone. In the largest study to date, no significant progression of fibrosis was observed in 56 patients (11 seronegative for hepatitis C), with liver biopsy specimens obtained before and after treatment with deferiprone at a mean interval of 3.1 years.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


