The Weiss scoring system is the most popular system used in the histologic diagnosis of adrenocortical carcinoma (ACC) and includes assessment of diffuse architecture; clear cells; nuclear grade; mitotic rate; atypical mitotic figures; necrosis; and venous, sinusoidal, or capsular invasion. However, it presents several limitations, including classification of borderline adrenal tumors (Weiss score of 3) or oncocytic and myxoid adrenal tumors. Oncocytic adrenocortical tumors demonstrate cells with eosinophilic cytoplasm, clear cells <25% of tumor volume, high-grade nuclear atypia, and diffuse architecture—all features diagnostic of ACC based on the Weiss scoring system and thus potentially misclassified. Oncocytic adrenocortical tumors are thus classified based on the Lin-Weiss-Bisceglia system that includes (1) major criteria (mitotic rate >5 mitoses/50 high-power fields, atypical mitoses, venous invasion)and (2) minor criteria (tumor size >10 cm or mass >200 g, necrosis, capsular invasion, sinusoidal invasion). The presence of any one major criterion is diagnostic of the oncocytic ACC, and the presence of at least one minor criterion indicates oncocytic neoplasm of uncertain malignant potential. The absence of any major or minor criteria is diagnostic of adrenocortical oncocytoma. , Here we present a case of oncocytic ACC.
Case Report
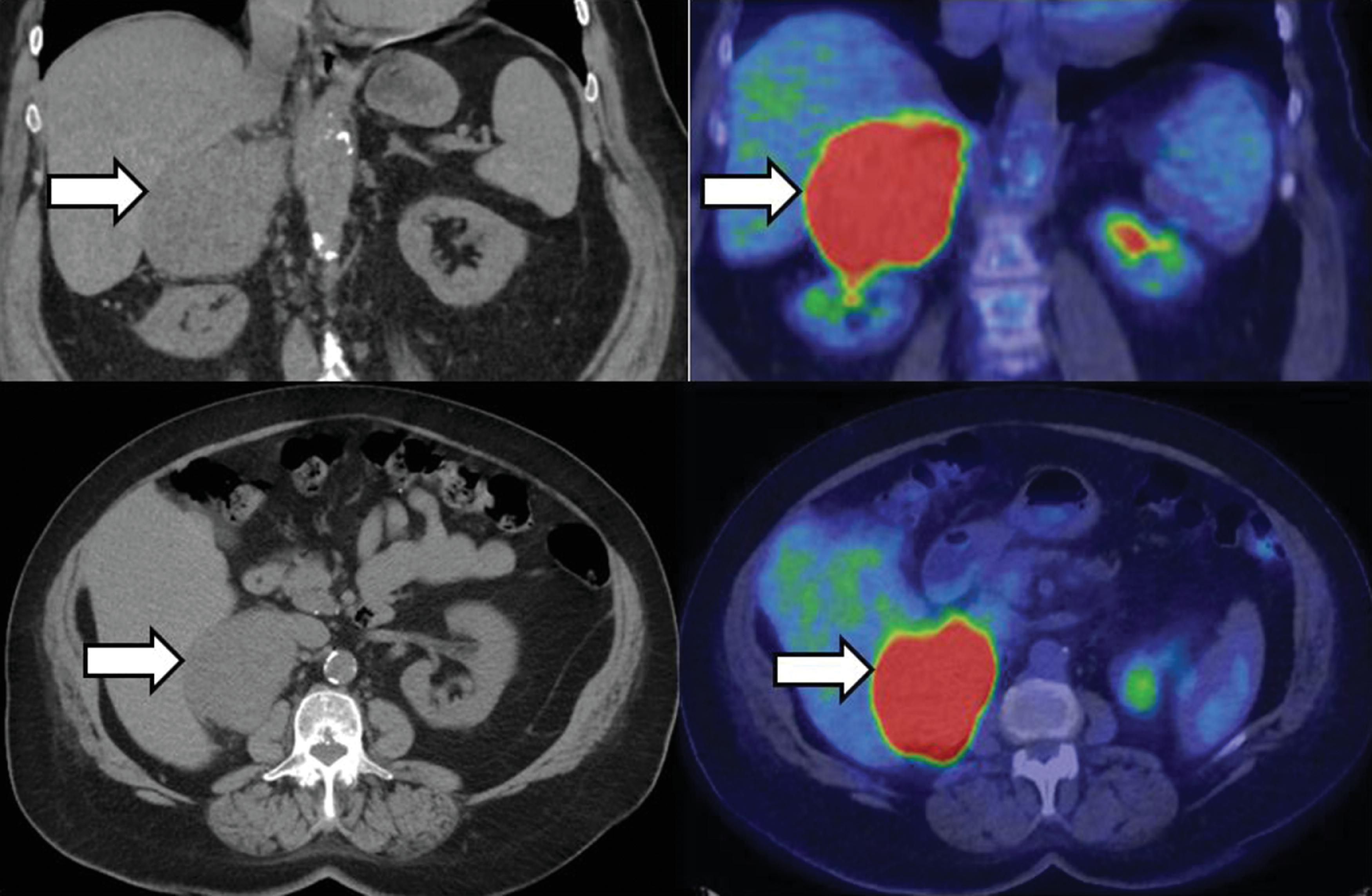
The patient was an 80-year-old woman incidentally discovered with a right adrenal mass during workup for acute abdominal pain, which was subsequently diagnosed as diverticulitis. Unenhanced computed tomography (CT) demonstrated a 8.2 × 7.1 × 6.3–cm right adrenal mass with an attenuation of 34 Hounsfield units (HU) ( Fig. 25.1 ). Initial workup locally included a 1-mg dexamethasone suppression test, which was normal (cortisol <1.4 mcg/dL). The patient was referred to Mayo Clinic for further management of the adrenal mass.
On evaluation, she did not notice any symptoms suggestive of androgen, cortisol, aldosterone, or catecholamine excess. However, she did note an unusual sensation in her both breasts that she thought was very similar to what she felt when breastfeeding years ago. She had long-standing hypertension and prediabetes, both stable. Her blood pressure was 142/82 mmHg, heart rate was 81 beats per minute, and body mass index was 38.44 kg/m 2 . Her only medication was losartan 75 mg daily.
INVESTIGATIONS
Laboratory evaluation showed normal levels of urinary metanephrines and normetanephrine; however, serum concentrations of progesterone and estradiol were higher than expected for the patient’s postmenopausal status ( Table 25.1 ). Positron emission tomography (PET) scan demonstrated intense F-18 fluorodeoxyglucose (FDG) uptake in the adrenal mass without any other foci of activity (see Fig. 25.1 ).
Related posts:
 45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
 Adrenocortical Carcinoma Associated With Multiple Endocrine Neoplasia Type 1
Adrenocortical Carcinoma Associated With Multiple Endocrine Neoplasia Type 1
 Cryoablation Therapy for Metastatic Paraganglioma
Cryoablation Therapy for Metastatic Paraganglioma
 Cushing Syndrome in the Setting of Multiple Endocrine Neoplasia Type 1
Cushing Syndrome in the Setting of Multiple Endocrine Neoplasia Type 1
 A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
 Catecholamine-Secreting Paraganglioma in Pregnancy
Catecholamine-Secreting Paraganglioma in Pregnancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


