CHAPTER 38 Onchocerciasis
Epidemiology
Almost 18 million people worldwide are infected with Onchocerca volvulus; almost 2% of those are blind, and another 3% have severely impaired vision. Almost all cases (99%) of onchocerciasis occur in sub-Saharan Africa, with about half of the cases found in Nigeria and Democratic Republic of Congo (Fig. 38.1). Onchocerciasis is a major public health problem along rivers where black flies breed, and where in some villages close to 100% of individuals may be infected. DNA probes have demonstrated the presence of different strains of the parasite. Blindness occurs more frequently with savanna strains of O. volvulus, while forest strains cause blindness less frequently even in heavily infected individuals. Infection is also present in Yemen and Saudi Arabia, though cases in the latter country are likely imported, as no transmission has been documented there. Onchocerciasis control programs have reduced disease burden in the Volta River Basin in West Africa and eliminated the disease from western Kenya.1
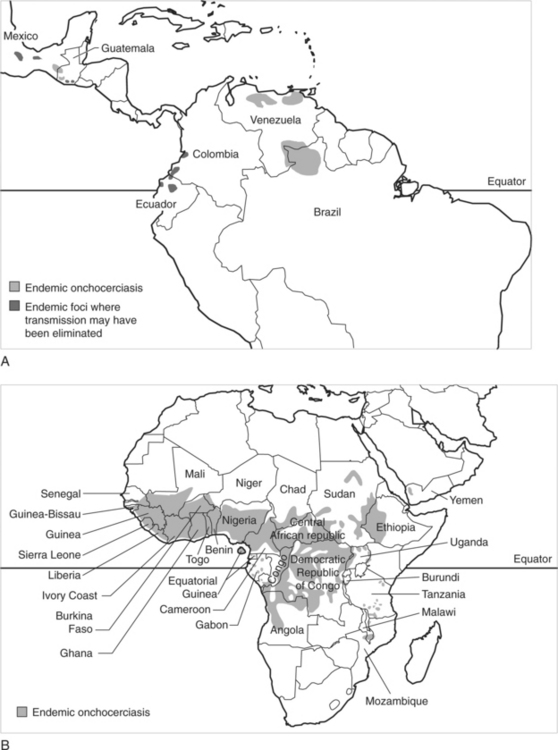
Fig. 38.1 Distribution of onchocerciasis. (A) Latin America. (B) Africa and the Middle East.
(Freedman D. Onchocerciasis. In: Guerrant RL, Walker DH, Weller PF, eds. Tropical infectious diseases. 2nd edn. Philadelphia: Churchill Livingstone; 2006:1178)
Isolated foci of onchocerciasis occur in the Americas, the largest of which are in Guatemala, Mexico, and Venezuela. Transmission is about 10-fold less intense in Central and South America than in sub-Saharan Africa, with comparatively lower worm burdens and lower rates of blindness. In contrast to the relative stability of disease distribution in Africa, where vector distribution determines that of the disease, foci in the Americas are enlarging as human habitation expands to rainforest areas where the Simulium vector is already present.1,2
Etiology
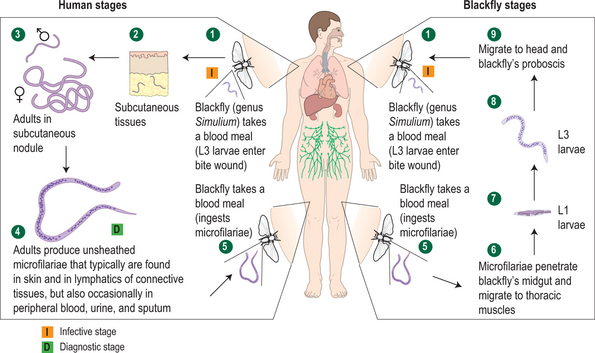
Onchocerca larvae are transmitted by the bite of the Simulium fly. The larvae are deposited into the skin where they require at least 6–12 months and a series of molts for development of mature adult worms, with the female worms capable of producing microfilariae. Adult females live inside fibrous nodules located subcutaneously or in deep musculature, while the smaller adult males appear to circulate from nodule to nodule to inseminate the females.1,2 Adult females may live as long as 14–15 years, producing hundreds of microfilariae each day. Microfilariae, whose lifespan ranges from 6 to 24 months, migrate from the nodules most commonly to the skin and the eye, but may also be found in lymphatic vessels and lymph nodes (Fig. 38.2). The Simulium fly ingests microfilariae present in the skin when taking a blood meal.
Clinical Manifestations
The clinical spectrum of disease due to Onchocerca volvulus is largely due to inflammatory responses to dying or dead microfilariae. No overt clinical disease is present in many infected individuals. In others, disease may involve the eye, the skin, and the lymph nodes. Short-term exposure rarely results in clinical manifestations of disease; symptoms may not appear until at least 2 years of exposure have occurred and the sole manifestation may be dermatitis.3 Clinical manifestations in those from endemic areas are a result of the interaction of duration of exposure, parasite burden, and host immune response.
Dermatitis
Skin lesions are the most common clinical manifestations of onchocerciasis. Itching is the most common complaint, and may be intense and profoundly troublesome. Papular dermatitis may occur along with itching, and may be localized to one part of the body or may be associated with swelling or edema.4 Recently, development of a classification scheme for dermatitis associated with onchocerciasis has facilitated communication about dermatologic manifestations of the disease.5 Patients may have manifestations in more than one category. The categories are:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


