© Springer International Publishing Switzerland 2015
Jean-Pierre Droz, Bernard Carme, Pierre Couppié, Mathieu Nacher and Catherine Thiéblemont (eds.)Tropical Hemato-Oncology10.1007/978-3-319-18257-5_45Cancer of the Penis, Anus, and Vulva
(1)
Medical Oncology Department, University Hospital Pitié-Salpétrière, Paris, France
(2)
Radiation Oncology Department, Institut Paoli-Calmettes, Marseille, France
(3)
Radiation Oncology Department, University Hospital Saint Louis, Paris, France
1 Introduction
Cancers and precancerous lesions of the anus, vulva, cervix, and penis cancers are associated with human papillomavirus (HPV). A high incidence of HPV-related cancer among patients with HIV/AIDS has been reported probably due to a persistence of HPV infection among those patients. Indeed, patients with HIV/AIDS have 4.5 times higher risk of penile cancer, 29 times higher risk of anal cancer, and 6.5 times higher risk of vulvar/vaginal cancer in comparison with the general population [1]. Unlike cervical cancer which is a major public health issue in developing country, anal, penile, and vulvar cancers are rare diseases.
2 Anal Cancer
2.1 Epidemiology
While uncommon (0.43 % of all malignancies), the anal cancer is increasingly frequent, with an incidence increasing from 0.8 to 1.7 cases per 100,000 persons per year from 1975 to 2011, respectively, in the United States [2]. Squamous cell cancer (SCCA) is the most common histologic diagnosis (85 %), followed by adenocarcinoma (10 %). Cancers and precancerous lesions of the anus are associated with human papillomavirus (HPV), and since 2012, anal lesions are subclassified into anal intraepithelial neoplasia (AIN): AIN I would correspond to anal LSIL, and AIN II/AIN III would correspond to anal HSIL. The median age at diagnosis is 60 years. HPV is the most known risk factor associated with anal cancer, especially HPV16. Other well-identified risk factors were receptive anal sexual intercourses, high number of sexual partners, immunosuppression, and smoking. Among HIV-infected patients, it has been reported that lower CD4 counts were associated with anal intraepithelial neoplasia and antiretroviral therapy was associated with a decreased prevalence of AIN but not with a decreased prevalence of high-risk HPV [3].
2.2 Screening and Prevention
Although it is not a routine for the general population, screening by a digital anorectal examination has been recently recommended every 2 or 3 years for HIV population as well as a high-resolution anoscopy with cytological evaluation. However, high-resolution anoscopy with cytological evaluation is most often not available in developing countries.
It has been shown that quadrivalent HPV vaccine decreased by 50 % AIN incidence. HPV vaccination is now recommended in current practice for boys and girls in the United States. HPV vaccination is prohibitively expensive and inaccessible in most people living in developing countries.
2.3 Clinical Presentation, Staging
The clinical manifestations of anal cancer are frequently late and nonspecific, because often they are confounded with hemorrhoids. Symptoms are mainly represented by anorectal bleeding (45 %), followed by pain (30 %), but can be thin-caliber stools and changes in bowel movements. 20 % of patients are asymptomatic [4]. Anal cancers are currently staged according the tumor, lymph node, metastasis (TNM) staging system of the American Joint Committee on Cancer (AJCC), seventh edition [5].
2.4 Patterns of Extension and Prognosis
Anal cancer extension can be direct through adjacent structures, lymphatic (perirectal, pelvic, and inguinal lymph nodes) and hematogenously (liver, lung, etc.). Perirectal (N1) lymph node invasion is more frequent for tumors arising above the dentate line, whereas tumors below the dentate line spread to inguinofemoral (N2) lymph nodes. Lymph node positivity is directly related to the extent of invasion of the primary tumor. Male gender, tumor diameter, and positive lymph nodes were the three independent prognosis factors predicting worse overall survival and disease-free survival in the two major randomized trials [6, 7].
2.5 Treatment
2.5.1 Anal Margin Cancer
For patients with T1N0, well-differentiated anal margin cancer, wide local excision is the gold standard treatment.
Patients with T2 or greater lesions should be treated with chemoradiation as anal canal cancers.
2.5.2 Anal Cancer
Localized Disease
Surgery
Since the development of chemoradiation regimens, APR which was the standard of care in the past decades should be reserved for salvage therapy after local relapse (10–30 % of cases) and/or for T4 lesions that did not achieve complete response after primary radiochemotherapy.
Radiotherapy
Exclusive radiotherapy is indicated for patients with T1N0 anal cancer.
Chemoradiation
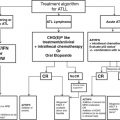
Two large randomized trials have demonstrated the superiority of chemoradiation over radiotherapy alone, in terms of progression-free survival and locoregional control [8, 9]. Another randomized trial demonstrated the interest of the use of mitomycine C for patients with T3 or greater lesions, and this treatment represents actually the standard of care for such advanced lesions [10]. Actually, the standard of treatment is full dose of 5-fluorouracil and mitomycine C for patients with a normal blood sample and/or in HIV patients with more than 200 CD4/m3 and a reduction of the dose of mitomycine C (5 mg/m2) for patients with abnormal blood count and or less than 200 CD4/mm3 [10]. The use of cisplatin instead of mitomycine C, as well as induction and maintenance chemotherapy, has been disappointing [11, 12].
Metastatic Disease
There is no consensus on chemotherapy regimens regarding metastatic anal cancer, but the most commonly regimen used is 5-fluorouracil plus cisplatin [13].
3 Penile Cancer
3.1 Introduction
Penile cancer is a rare disease and mainly affects elderly patients. It is associated with human papillomavirus (HPV) infection which is present in 15–80 % of patients. HPV 16 and HPV 18 are the most common serotypes (60 % and 13 %, respectively).
Incidence of penile cancer is much higher in low and middle income countries than in Western countries. The disease frequently develops in men of low socioeconomic status and poor standards of penile hygiene [14]. Incidence is less than 1/100,000 males in Western countries, 3/100,000 in rural India, and 8.3/100,000 in Brazil. Uganda is the country with the highest cumulate rate of penile cancer (1 % by age 75 years). 95 % of penile cancers are squamous cell cancers.
3.2 Prevention
It has been shown that circumcision protects against penile cancer. Neonatal circumcision reduces the risk of penile cancer by at least ten times [15], and circumcision in the childhood reduces the risk by 3–5 times. Adult circumcision does not protect against penile cancer.
3.3 Treatment
3.3.1 Localized Disease
Cancer In Situ and Noninvasive Verrucous Cancer
Circumcision followed with 5-fluorouracil topical treatment if the lesion was not completely excised by the biopsy is indicated.
Persistent lesion could be treated with topical 5 % imiquimod as second-line treatment.
Surgical excision is reserved for refractory or extensive lesions.
Invasive Cancer
For distal penile T1 tumor, conservative surgery with partial penectomy is indicated. Conservative external beam radiotherapy or interstitial brachytherapy after circumcision is also an effective treatment in penile cancer, for tumor less than 4 cm without corpus cavernosum infiltration.
For proximal penile T1 or tumor with less than 2 cm margins, total penectomy with perineal urethrostomy is recommended.
For T4 tumor, emasculation consisted with penectomy, scrotectomy, and bilateral orchidectomy is recommended.
For nonresectable T4 tumor or fixed lymph node, neoadjuvant chemotherapy or concomitant chemoradiotherapy could be proposed before surgery.
Lymph Node Management
Penile cancer is a lymphophilic tumor. Prophylactic elective lymph node dissection is recommended in T2, T3, or T4 and/or high-grade tumors.
Inguinal lymphadenectomy is indicated in case of palpable inguinal lymph nodes. It is important to note that lymphadenectomy is curative in only 50 % of cases.
Postoperative radiation is indicated in patients with positive surgical margin, extensive lymph node metastasis, extracapsular lymph node spread, or pelvic lymph node involvement.
For pN2 or pN3 disease, adjuvant chemotherapy could be proposed after tumor resection and lymphadenectomy.
3.3.2 Metastatic Disease
Several chemotherapy drugs such as 5-fluorouracil, cisplatin, methotrexate, or bleomycin have been shown to be active in penile cancer.
Chemotherapy in penile cancer is delivered as palliative treatment.
4 Vulvar Cancer
4.1 Epidemiology
Vulvar cancer is a relatively rare disease. With 27,000 new cases worldwide for a year, age-adjusted incidence is 0–4.6 /100,000. Lower rates are observed in Asia and Africa than in other parts of the world. It represents less than 5 % of gynecologic malignancies [16, 17]. Vulvar squamous cell cancer (VSCC) represents more than 90 % of the tumor. Morphological variants have been described including keratinizing, basaloid, warty, and verrucous cancer.
Human papillomavirus (HPV) DNA prevalence varies from 20 to 40 % [18, 19], and two pathways are distinguished: HPV-dependant and HPV-independent tumor [20]. In the first group, HPV 16 represents 75 % of the cases and usually is related to usual vulvar intraepithelial neoplasia (uVIN) as precursor. During last decades, VIN incidence increases. The risk of transformation toward VSCC represents approximatively 10 % of the case and only 3 if VIN had been treated. This pathway is associated with younger age, smoking, high sexual partner number, and compromised immune status [20–22]. The HPV-independent type is more often associated with p53 mutation. It occurs mainly in older women and is associated with lichen sclerous or chronic dermatosis with autoimmune diseases. Differentiated VIN (dVIN) is considered as the precursor and has a higher progression risk toward VSCC. Prognosis seems to be worse than HPV-dependent cancer [20–22].
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


