Chapter 60 Noninvasive Breast Cancer
Lobular Carcinoma in Situ
Lobular carcinoma in situ (LCIS) was first described as a pathologic entity by Foote and Stewart in 1941.1 Microscopically, LCIS appears as a noninfiltrating process of lobular proliferation. LCIS has been reported to present with multicentric breast involvement in up to 90% of mastectomy specimens, with bilateral involvement documented in 35% to 59%.2–5 Histologically, LCIS is characterized by loose discohesive epithelial cells filling the acinar space.2–5 The degree of lobular involvement ranges from a simple filling of the ductal lumens to moderate distention to overt distention with extension into the adjacent extralobular ducts.6 As a result of this spectrum of appearances, the lines of histologic delineation can become blurred between atypical ductal hyperplasia, LCIS, and, when ductal extension is seen, DCIS. This introduces a source of complexity when comparing publications from varying institutions.3–5
Molecular markers have been suggested as a potential method of providing a technique for distinguishing LCIS in problematic cases.4 LCIS cells are frequently ER-positive cells, and rarely is c-ERBB2 overexpressed or the TP53 protein accumulated.4,7–9 The loss of E-cadherin (CDH1) gene expression is documented in more than 95% of LCIS cases.9,10 The E-cadherin gene is a calcium-dependent cellular adhesion molecule that is responsible for epithelial organization, and the absence of this adhesion molecule in LCIS may explain its discohesive morphologic characteristics.9,10
Publications on biopsy results report LCIS incidence rates to be 0.5% to 3.6%; these lesions represent less than 15% of all noninvasive lesions recorded.5,11 Because there are no clinical or mammographic indicators, LCIS without additional histologic findings is typically an incidental finding when biopsy is performed for alternative reasons.1–411 Although mammographically detected calcifications corresponding with LCIS have been reported, the calcifications are more commonly unassociated and are present in the adjacent tissue.12 In fact, DCIS or invasive disease, or both, is frequently identified in the subsequent lumpectomies performed (22% to 27% of cases) when LCIS is the sole histologic entity seen on core biopsy.13,14 Criteria identifying those patients for whom observation only is sufficient following core biopsy showing LCIS have not yet been clearly specified.
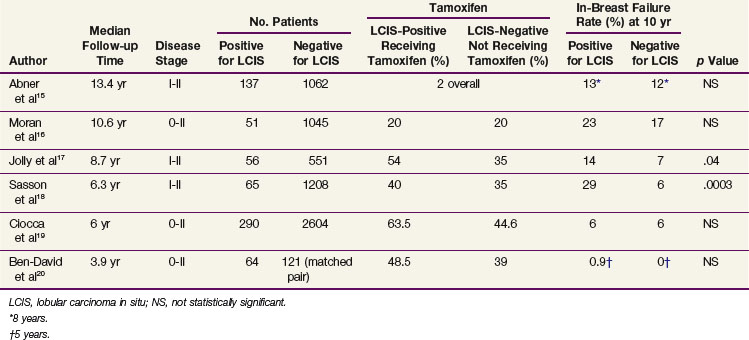
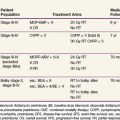
Management considerations for LCIS differ depending on whether it is associated with a diagnosis of DCIS or infiltrative disease or whether LCIS is the sole histologic entity encountered. Only 5% to 12% of early-stage breast cancers have an associated component of LCIS.15,16 Several institutional experiences have evaluated the potential impact of the presence of LCIS on breast-conserving treatment outcomes.15–20 The number of patients included in these experiences are relatively small, and there are differences in these cohorts, including pathologic assessment, length of follow-up, and use of tamoxifen (Table 60-1). However, the majority of data suggest that no statistically significant difference exists when comparing rates of in-breast disease control, distant disease-free survival, and overall survival between patients with or without a component of LCIS.15–20 The presently accepted treatment approach is to manage the breast according to the dominant histologic findings present (DCIS or invasive disease) and disregard the presence of LCIS. Additional surgery is not pursued to obtain LCIS clear margins. The need for the addition of tamoxifen and/or a more aggressive treatment approach in this group of high-risk patients is uncertain, and further study is necessary.
If LCIS is the sole histologic diagnosis, treatment recommendations range from observation to mastectomy. When first described as a pathologic entity, the significance of LCIS was unknown and mastectomy was consistently pursued.1 Knowledge of frequent contralateral involvement extended treatment recommendations to random contralateral biopsy and bilateral mastectomy.1,2 However, observational studies after lumpectomy only have led to a better understanding of the natural history of this disease, and a more conservative approach is now commonly practiced.5,11 Although studies of E-cadherin (CDH1) and loss of heterozygosity (LOH) suggest that LCIS may be a precursor to invasive disease, LCIS has historically been considered a marker for an increased risk of developing invasive disease (9 to 12 times that of the normal population); this risk requires long-term follow-up exceeding 20 years.3,12
A range of ipsilateral and contralateral breast failure rates are reported. This variation is due in part to differences in the length of follow-up, the definitions used for histologic classification (atypical lobular hyperplasia vs. LCIS), and the extent of excision used in these observational studies.21,22 In a recent 12-year follow-up publication on a 182-patient cohort treated with lumpectomy only for LCIS, the National Surgical Adjuvant Breast and Bowel Project (NSABP) reported a 14.4% in-breast tumor recurrence (IBTR) rate and a 7.8% contralateral breast tumor recurrence (CBTR) rate.22 Of the IBTRs, nine (34.6%, or 5% of the total cohort) were invasive malignant tumors and 17 (65.4%, or 9% of the total cohort) were noninvasive malignant tumors. Although the frequency of CBTRs was less than that of IBTRs, the frequency of invasive CBTRs (5.6% of the total cohort) was similar to that of invasive IBTRs (5% of the total cohort). All of the IBTRs were documented to be at the site of the index lesion except for one, characterized as pure LCIS, that was found at a remote site. This report continues to support the indolent nature of LCIS and a conservative management approach.
The impact of subsequent development of invasive disease on mortality risk has been estimated in earlier publications to be 5% to 7%.11 However, with contemporary use of close mammographic and clinical follow-up leading to early detection of subclinical abnormalities, one would expect this mortality risk to be reduced. This reduction is reflected in the lower mortality risk (1%) reported by the NSABP.22
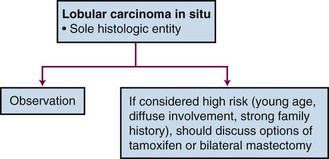
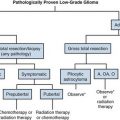
Management options vary depending on individual risk assessment (Fig. 60-1). Close observation with regular physical examinations and mammographic surveillance is the accepted management approach.5,11,21,22 At present, there is no role for radiotherapy in the management of LCIS. Knowing that this is a bilateral breast disease process leaves a unilateral treatment approach inadequate (i.e., ipsilateral mastectomy). Bilateral prophylactic mastectomy is thought to be excessive in all patients except those believed to be at higher risk (i.e., young patients, diffuse process, a significant family history of disease) for whom it could be considered. A less radical approach to be considered is the use of tamoxifen. Indeed, a cohort of patients with LCIS were entered into the NSABP P-01 trial, which compared tamoxifen with placebo for breast cancer prevention. The 5-year risk of subsequent disease development was reduced with the use of tamoxifen by 56%.23
Paget’s Disease
The clinical presentation of crusting, bleeding, and ulceration of the nipple was first described in 1856, but it was not until 1874 that the association with an underlying breast carcinoma was recognized by Sir James Paget.24,25 Paget’s disease of the nipple is characterized histologically by the presence of unique, clearly identifiable Paget’s cells that are described as large, round to oval cells that contain hyperchromatic nuclei and prominent nucleoli. Mitoses are frequently seen. The Paget’s cells occur singly or in clusters and are scattered throughout the epidermis.26–28
Reported in 0.5% to 5% of breast cancer patients, Paget’s disease is an infrequent diagnosis.26,29,30 It is most commonly unilateral, but reports of bilateral and male Paget’s disease can be found.31–33 Clinically, women describe itching and burning of the nipple and areola and crusting is often described. There is a slow progression toward an eczematoid appearance, which can extend to the skin. If neglected, bleeding, pain, and ulceration can occur.30 The differential diagnosis includes superficial spreading melanoma, pagetoid squamous cell carcinoma in situ, and clear cells of Toker.27,28 A palpable mass is detected in about 50% of patients at diagnosis. If there is a palpable mass, more than 90% will be invasive carcinoma. On the other hand, if no palpable mass is detected, 66% to 86% will have an underlying DCIS. These adjacent, underlying malignant tumors are usually located centrally; however, they have also been located elsewhere in the breast.26,30
The appropriate management of Paget’s disease remains unsettled; however, in concordance with physician and patient preference, attempts have been made to investigate the role of breast-conservation therapy. Because mastectomy was initially shown to be effective, the transition to breast-conserving treatment has been cautious due to the inability to accumulate a significant number of uniform patients similarly treated.29,30 Limited series have described results with various forms of breast-conserving treatment, including limited surgical resection alone, radiotherapy alone, and limited resection followed by radiotherapy34–39 (Table 60-2).
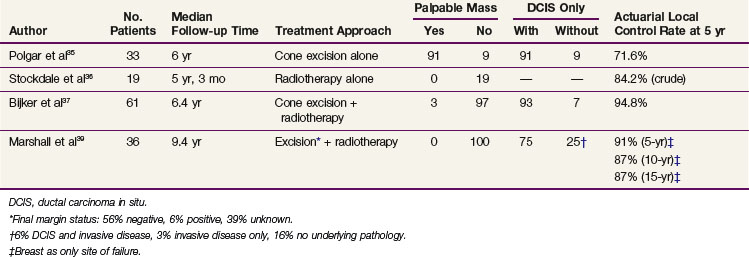
The combination of limited surgical resection and postoperative radiotherapy appears to be the most successful breast-conservation approach. Two collaborative studies have shown the successful use of breast-conservation therapy in Paget’s disease of the nipple. The European Organization for Research and Treatment of Cancer (EORTC) Study 10873 was a multi-institutional registration study reporting a 5-year local recurrence rate of 5.2%.37 In this study, a complete excision with tumor-free margins of the nipple-areolar complex and underlying breast tissue was followed by whole-breast radiotherapy to 50 Gy. The median follow-up time was 6.4 years, and the majority of patients were found to have an underlying DCIS without a palpable mass.
The second study, a seven-institution collaborative review of 36 patients, included patients with Paget’s disease without a palpable mass or mammographic density.39 The median follow-up time was 9.4 years, and all had at least 12 months of follow-up. Patients underwent complete (69%) or partial (25%) excision of the nipple-areolar complex and underlying breast tissue, with 6% reported as a biopsy only. The final margin status was documented as negative in 56%, positive in 6%, and unknown in 39%. All received whole-breast irradiation at a median dose of 50 Gy, and the majority received an additional boost dose to the tumor bed. Actuarial rates of local in-breast failure as the only site of first recurrence were 9% at 5 years and 13% at both 10 years and 15 years. Despite the variation of clinical, pathologic, and treatment factors, statistical evaluation did not identify any factors that significantly predicted for risk of local recurrence.
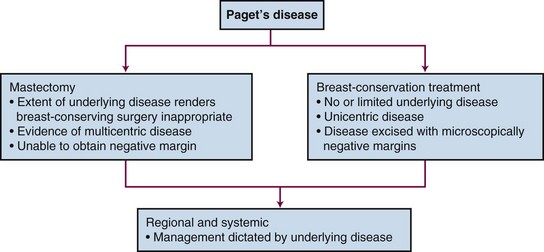
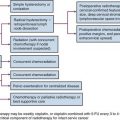
On presentation, the workup and evaluation should include a bilateral breast examination, mammography, and biopsy to confirm the diagnosis of Paget’s disease and fully evaluate the extent of the underlying malignant disease. An individual’s prognosis is not dependent on the diagnosis of Paget’s disease but rather depends on the associated underlying malignant disease. Therefore local treatment decisions as well as systemic and regional nodal disease risk management should be based on the underlying disease (Fig. 60-2). Standard breast-conservation therapy principles governing patient selection, surgical resection, and radiotherapy should be applied. Complete surgical resection of the disease process (i.e., nipple-areolar complex excision in conjunction with any underlying disease) with a negative microscopic surgical margin is then followed by standard whole-breast irradiation.
Ductal Carcinoma in Situ
Epidemiology
Ductal carcinoma in situ (DCIS) is represented by a heterogeneous spectrum of histologic appearances that all arise within and are confined to the ductal lumens of the breast. This clonal proliferation does not breach the epithelial basement membrane, and there is no evidence of invasion into the adjacent breast stroma.40 DCIS lacks the ability to metastasize; the rarely reported axillary nodal metastasis or distant metastasis has been attributed to the probable presence of an undetected component of invasive carcinoma.40
Before 1980, the incidence of DCIS was low (i.e., only 1.4% of all breast biopsies and only 5% of all breast malignant tumors).41,42 With the increased use of mammography and as pathologists began to recognize that DCIS was a distinct pathologic entity, the incidence of DCIS dramatically increased.43,44 The incidence of DCIS increased from 4800 cases reported in 1983 to more than 50,000 cases reported in 2003; this represents a 10-fold increase in only 20 years.40,45 Of the estimated 192,370 new breast cancers diagnosed in 2009, 62,280 will be noninvasive, of which 85% will be DCIS.46 With this increase, there has been a corresponding change in the presentation of DCIS lesions from predominantly palpable to more than 90% of new lesions being nonpalpable.45 Studies have shown that the rate of DCIS lesions detected by screening increases with age, whereas DCIS accounts for a progressively smaller percentage of the total cancers detected (i.e., invasive cancers plus DCIS).47,48 The rate of DCIS detection has been shown to increase from 0.56 per 1000 mammograms among women aged 40 to 49 years to 1.07 per 1000 mammograms among women aged 70 to 84 years.48
Associated risk factors for the development of DCIS are similar to risk factors for invasive disease and include older age, benign breast disease, a family history of disease, and reproductive factors, including nulliparity or older age of pregnancy.40,49–51
Prevention and Early Detection
Although successful treatment options are in use, improved outcomes can be realized through both prevention of DCIS development and the early detection of new lesions. The role of tamoxifen in the prevention of disease development has been studied by the NSABP in a protocol that randomized patients at high risk for the development of breast cancer to either tamoxifen or placebo.23 Patients eligible included those who were either 60 years of age or older, had a history of LCIS, or were between the ages of 35 and 59 years with a 5-year predicted risk for breast cancer, using the Gail model, of at least 1.66%. The 5-year follow-up data reveal that for noninvasive breast cancer, tamoxifen use was associated with a 50% reduction in risk. The average annual rate of noninvasive breast cancer per 1000 women was 2.68% in the placebo group compared with 1.35% in the tamoxifen group, yielding a relative risk (RR) of 0.50 (95% CI, 0.33 to 0.77).23
Mammography plays an essential role in the early detection of noninvasive lesions, providing an opportunity for intervention early in the course of disease development. The distinctive mammographic feature of DCIS is the presence of microcalcifications, which has been reported in 84% to 98% of cases.52,53 Seventy-two percent to 76% of DCIS lesions have microcalcifications as the sole mammographic finding, and an additional 12% have microcalcifications in combination with other mammographic abnormalities.52,53
Beyond detection, several attempts have been made to correlate the mammographic appearance of the lesion with the histologic type, grade, and extent of disease. Linear branching microcalcifications have been reported to be associated with high-grade or comedo-type DCIS. Heterogeneous granular calcification is commonly associated with moderately differentiated DCIS and fine granular microcalcifications more typically with low-grade, noncomedo DCIS.48,52,53 Although there is a degree of correlation between appearance and histologic type, there is considerable overlap, which limits the use of this information in clinical decision making. Microcalcifications are not always present throughout the histologic abnormality, and the estimated mammographic size and extent of disease frequently underestimate the true pathologic extent of the disease process. Although the mammographic extent can be used to guide the extent of surgical excision, caution should be exercised because the size is typically underestimated by 1 to 2 cm.54,55 In patients presenting with nipple discharge with a negative mammographic evaluation, galactography may be helpful in distinguishing the presence of a papilloma from an underlying DCIS.56
Biologic Characteristics and Molecular Markers
DCIS is a precursor lesion to invasive ductal carcinoma and exists along an evolutionary continuum that starts with benign breast tissue and ends with an invasive breast lesion.57 This concept has been verified in several ways. For years, pathologists have recognized and documented confirmation of a histologic progression from benign breast cells to invasive breast cancer and realized that this histologic evidence was more commonly present where an invasive lesion was discovered. The evolutionary concept is further supported by the acknowledged association between the presence of DCIS and the subsequent increased risk of developing an invasive breast cancer.40,58,59 In some series, a 10-fold risk of developing an invasive lesion has been reported. The presence of shared identical genetic abnormalities between DCIS and synchronous invasive breast cancer demonstrates a clonal relationship of biologic progression.40,58–60
Documented genetic and molecular differences can differentiate DCIS from normal breast tissue. Genetic alterations have been evaluated with an analysis of LOH that has demonstrated gain or loss of multiple loci.58–60 LOH is not seen in normal breast tissue but is present with an increasing frequency that correlates with histologic progression from benign to malignant tissue. In hyperplasias from noncancerous breasts, LOH is rarely documented; however, it is more commonly present (in 42% to 50% of patients) in atypical ductal hyperplasia. Among specimens harvested from cancerous breasts, 77% of noncomedo and 80% of comedo DCIS lesions share LOH with the synchronous invasive lesion in at least one locus.60 Molecular markers have been studied and are found to have a heterogeneous distribution of expression.40 The ER is present in 70% of DCIS lesions, but the rate of expression is high (90%) in low-grade lesions and is significantly less (25%) in high-grade lesions. This trend is reversed with the HER2/neu proto-oncogene and the TP53


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


