more intense smoking, as it changes the aroma of the smoke and decreases the irritant effect of the smoke, thereby facilitating more intense inhalation.18,19
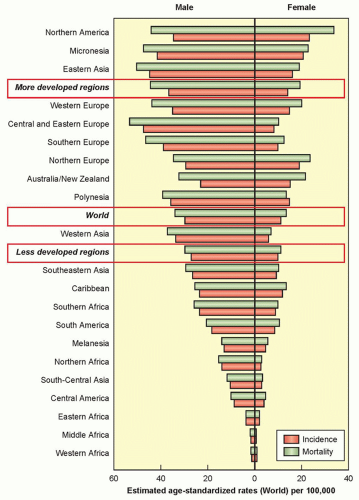 Figure 37.1 Estimated age-standardized rates of lung cancer per 100,000 population by region of the world. (Reproduced from GLOBOCAN 2012, International Agency for Research on Cancer, World Health Organization.) |
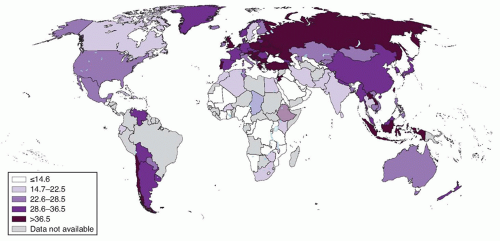 Figure 37.2 Percentage of tobacco use among adults by country in 2005. (Reproduced from GLOBOCAN 2012, International Agency for Research on Cancer, World Health Organization.) |
with an increase in lung cancer risk. In particular, patients with idiopathic pulmonary fibrosis have been reported to have an odds ratio for lung cancer of 8.25 compared to controls.50,51 In contrast to COPD, cigarette smoking is usually not etiologically implicated in interstitial diseases, although chronic inflammation typically is felt to contribute to the pathologic process.
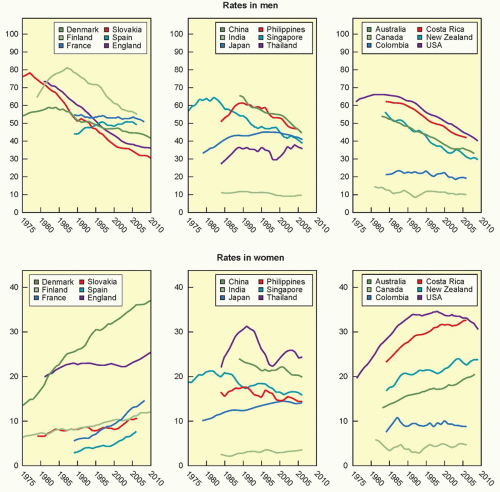 Figure 37.3 Trends in mortality from lung cancer showing the age-standardized mortality rate from lung cancer per 100,000 men (top row) and women (bottom row) in selected countries. (Reproduced from GLOBOCAN 2012. International Agency for Research on Cancer, World Health Organization.) |
of the impact of that tumor characteristic. Because the database consisted of patients diagnosed between 1990 and 2000, advances in technology (e.g., PET imaging) and treatment modalities that are routine today are not reflected. The analysis did not account for what treatment (if any) was given. In fact, there was a great deal of variation in outcomes depending on the type of source data and the geographic region. Thus, while the outcomes created a phenomenal tool to define where to draw distinctions between TNM categories and groupings, the outcomes themselves represent a global cross-section from the past with less clear relevance to specific patients today.
TABLE 37.1 Stage Classification: T, N, M Descriptors | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
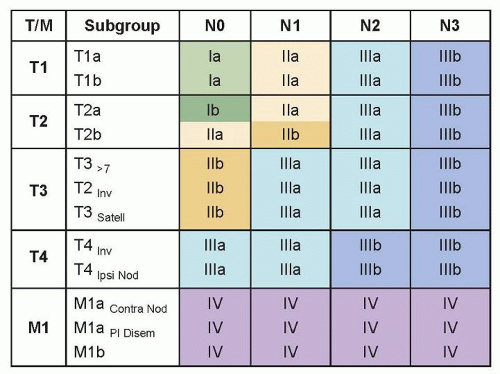 Figure 37.4 Stage classification: Stage groups. Inv, invasion; Satell, satellite; Ipsi Nod, ipsilateral nodule; Contra Nod, contralateral nodule; Pl Disem, pleural dissemination. (Reproduced with permission from Detterbeck F, Tanoue L, Boffa DJ. The new lung cancer staging system. Chest 2009;136:262.) |
TABLE 37.2 International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society Classification of Lung Adenocarcinoma in Resection Specimens | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||
TABLE 37.3 Genetic Alterations in Non-Small-Cell Lung Cancer | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
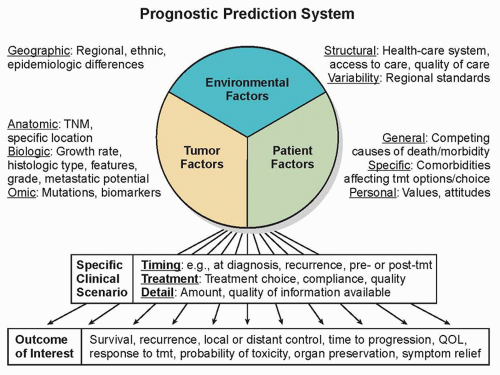 Figure 37.5 Schematic of a prognostic prediction system, taking into account environmental, patient-related, and tumor-related factors. The prediction must be specific to the clinical scenario and the outcome of interest. TNM, tumor, node, metastases; QOL, quality of life; tmt, treatment. |
2 weeks) before undergoing surgery; pharmacologic interventions are safe to continue in the perioperative period as well.76 A wellorganized thoracic oncology program, therefore, should include an evidence-based smoking cessation program that is fully integrated with the diagnostic and treatment components of patient care.
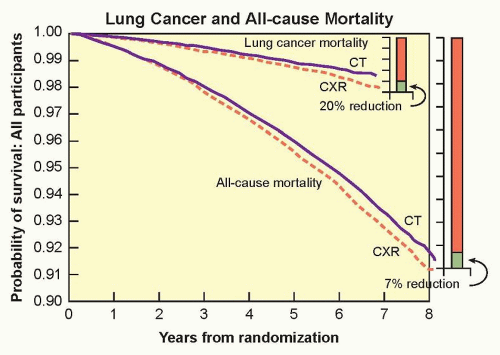 Figure 37.6 Lung cancer mortality and overall mortality reduction by computed tomography (CT) screening in the National Lung Screening Trial. CXR, chest X-ray. Data taken from Aberle D, Adams A, Berg C, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Eng J Med 2011;365:395-409. |
required, the number of follow-up imaging exams, the number of overdiagnosed lung cancers, and radiation-related lung cancer deaths. Based on the models, a range of different screening scenarios are arguably valid, with different balances of benefits and harms, with the most efficient screening projected in a population similar to the NLST. On the basis of the Cancer Intervention and Surveillance Modeling Network analysis, the US Preventative Services Task Force now recommends “annual screening for lung cancer with low-dose computed tomography in adults ages 55 to 80 years who have a 30 pack-year smoking history and currently smoke or have quit within the past 15 years.”101
biopsy or observation. False-positive PET results may occur with any inflammatory or infectious process: tuberculosis, fungal infections, rheumatoid nodules, and sarcoidosis—when such a process is suspected, PET is generally not helpful (it does not differentiate between such a process and cancer). PET also carries a high false-negative rate with ground glass opacities (GGO), carcinoid tumors, or small lesions; in these situations, PET should also generally be avoided. Specifically, the false-negative rate of PET in a GGO is approximately 90%.118 The false-negative rate in solid lesions <1.5 cm is ˜15% and in lesions <1 cm ˜30% to 50%.118 Although the “resolution” of modern PET scanners is ˜6 mm, this is a technical and not a clinical term—a lesion must have a diameter of four times the resolution in order to detect >90% of the 18-fluorodeoxyglucose activity that is present. This fact also explains why the detected standard uptake value of a lesion falls linearly for lesions smaller than ˜2 cm, even if the actual amount of 18-fluorodeoxyglucose activity remains the same.118,120
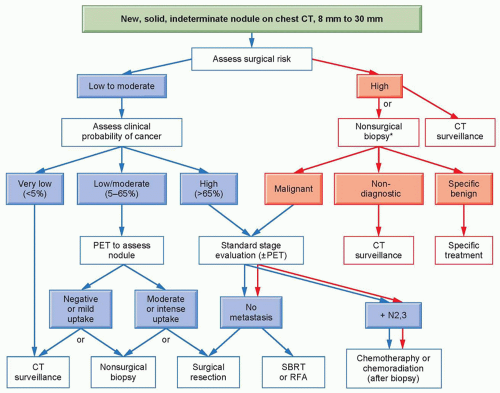 Figure 37.7 Management algorithm for individuals with solid pulmonary nodules 8 to 30 mm in diameter. Branches indicate steps in the algorithm following nonsurgical biopsy. *Among individuals at high risk for surgical complications, we recommend either computed tomography (CT) scan surveillance (when the clinical probability of malignancy is low to moderate) or nonsurgical biopsy (when the clinical probability of malignancy is moderate to high). PET, positron emission tomography; SBRT, stereotactic body radiotherapy; RFA, radiofrequency ablation. (Reproduced with permission from the American College of Chest Physicians Lung Cancer Guidelines, Gould MK, Donington J, Lynch W, et al. Evaluation of individuals with pulmonary nodules: when is it lung cancer? Chest 2013;143:e93S-120S.) |
extrathoracic sites. Pathologic staging (identified by a “p” prior to the stage group) is determined only if surgical resection with intent to cure is performed. All patients undergo clinical staging; the subset of patients who have pathologic staging all first had a clinical stage defined that determined that a surgical resection was indicated. Pathologic staging is inherently more accurate than clinical staging; comparison of survival typically demonstrates better survival for pathologically as compared to clinically staged patients.52 Nonetheless, it is the clinical stage that drives the initial treatment decisions, and thus it is imperative that the process of defining the clinical stage be performed rigorously.
TABLE 37.4 Approach Diagnosis and Staging of Patients with Probable Lung Cancer | |||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||
conventional imaging.131,137 The ACCP and NCCN guidelines are relatively generic in recommending PET in essentially all patients with a suspected or diagnosed lung cancer, without accounting for details of the clinical stage before PET or the clinical setting (only cIa and GGO lesions are excluded from the PET recommendation by the ACCP).110,141
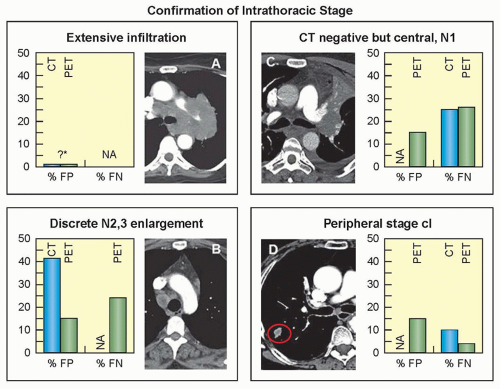 Figure 37.8 False-positive and falsenegative rates for computed tomography (CT) and positron emission tomography (PET) assessment of mediastinal nodes by the American College of Chest Physicians intrathoracic radiographic (CT) classification categories. ?*, estimated, no actual data available; NA, not applicable; % FP, percent of positive test results that are false positive (= 100 – positive predictive value%); % FN, percent of negative test results that are false negative (= 100 – negative predictive value %). (Reproduced with permission from the American College of Chest Physicians Lung Cancer Guidelines, Silvestri GA, Gonazalez AV, Jantz M, et al. Methods of staging for non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013; 143:e211S-e250S.) |
TABLE 37.5 Accessibility of Node Stations to Various Invasive Mediastinal Staging Techniques | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
in Asia.158 It is not clear what the reasons for these differences are. It is well known that the incidence of EGFR mutation is higher in the Asian lung cancer population. There are differences in the proportion of subtypes of NSCLC. There are societal differences regarding how aggressive and which treatment modalities are generally accepted. There are differences in the availability of various technologies and treatment methods (e.g., EBUS, PET, VATS, four-dimensional RT, stereotactic body RT [SBRT], genetic testing). The impact of these differences is not clear, but it does emphasize that general recommendations need to be thoughtfully considered in light of differences as compared with the population and setting in which the data was derived.
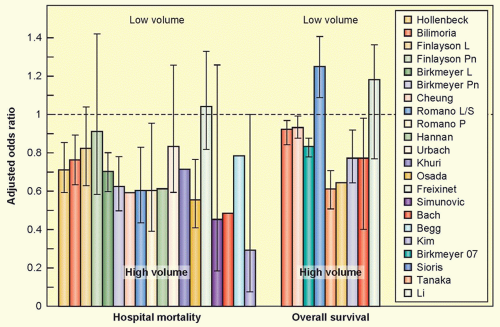 Figure 37.9 Surgical outcomes according to case volume. Perioperative mortality and long-term survival according to institutional case volume of patients undergoing surgical resection for lung cancer. (Data taken from Howington J, Blum M, Chang A, et al. Treatment of stage I and II non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013;143:e278S-313S.) |
history of myocardial infarction are rendered moot if a successful intervention for the coronary artery disease has been accomplished and overall cardiac function has been preserved. Thus, evaluation of which patients can safely undergo surgery, including VATS and sublobar resection, has become much more nuanced and is best approached in a multidisciplinary fashion, which should include a dedicated thoracic surgeon, a pulmonologist with knowledge about lung cancer treatment options, and a radiation oncologist as well.
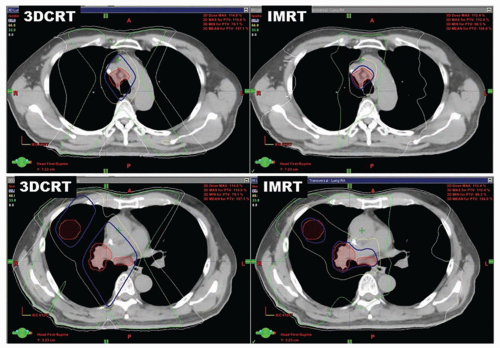 Figure 37.10. Radiation treatment plans: Comparison of two methods. A 64-year-old former smoker presented with stage IIIA non-small-cell lung cancer, with disease in the right lower lobe, hilum, and mediastinal station R4. Concurrent chemoradiation was recommended. Radiation plans were generated using three-dimensional conformal radiotherapy (3DCRT) and intensitymodulated radiotherapy (IMRT). Representative axial slices from the two plans are shown: the top panels compare 3DCRT (left) to IMRT (right) at the level of the aortic arch, the bottom panels are similarly presented for an axial level below the carina. The planning target volume is shown in red, isodose lines are demonstrated for 60 Gy (dark blue), 40 Gy (yellow), 20 Gy (green) and 5 Gy (white). The use of IMRT decreased the mean lung dose (16 Gy versus 13 Gy) and V20 (32% versus 23%), but increased the volume of lung receiving 5 Gy. The esophageal dose was also lower with IMRT; V30 was reduced from 41% to 23%. |
stenosis or fistula formation, is less common after conventionally fractionated radiation, occurring in <5% of patients.213,214
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


