This classification system applies to well‐differentiated neuroendocrine tumours (carcinoid tumours and atypical carcinoid tumours) of the gastrointestinal tract, including the pancreas. Neuroendocrine tumours of the lung should be classified according to criteria for carcinoma of the lung. Merkel cell carcinoma of the skin has a separate classification. High‐grade neuroendocrine carcinomas are excluded and should be classified according to criteria for classifying carcinomas at the respective site. The following grading scheme has been proposed for all gastrointestinal neuroendocrine tumours (carcinoids): Notes 1 10 HPF: high power field = 2 mm2, at least 40 fields (at 40× magnification) evaluated in areas of highest mitotic density. 2 MIB1 antibody; % of 500–2,000 tumour cells in areas of highest nuclear labelling. All Grade 3/high‐grade tumours should be classified according to criteria for classifying carcinoma at the respective sites. Note For any T, add (m) for multiple tumours.
WELL‐DIFFERENTIATED NEUROENDOCRINE TUMOURS OF THE GASTROINTESTINAL TRACT
Rules for Classification
Histopathological Grading
Grade
Mitotic count (per 10 HPF)1
Ki‐67 index (%)2
G1
< 2
≤ 2
G2
2–20
3–20
G3
> 20
> 20
Stomach
TNM Clinical Classification
T – Primary Tumour
TX
Primary tumour cannot be assessed
T0
No evidence of primary tumour
T1
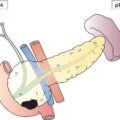
Tumour invades the mucosa or submucosa and is no greater than 1 cm in greatest dimension (Fig. 245)
T2
Tumour invades muscularis propria or is more than 1 cm in greatest dimension (Fig. 245)
T3
Tumour invades subserosa (Fig. 245)
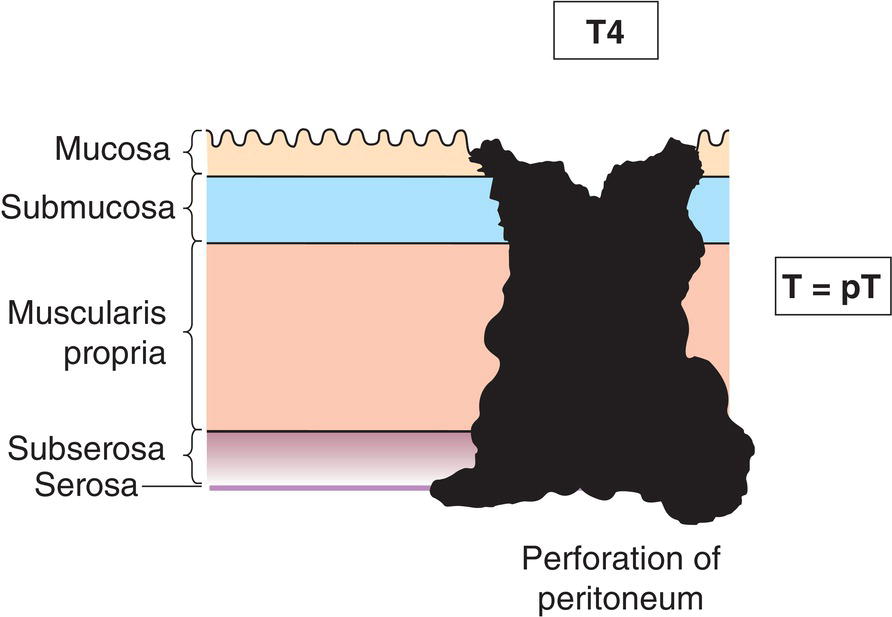
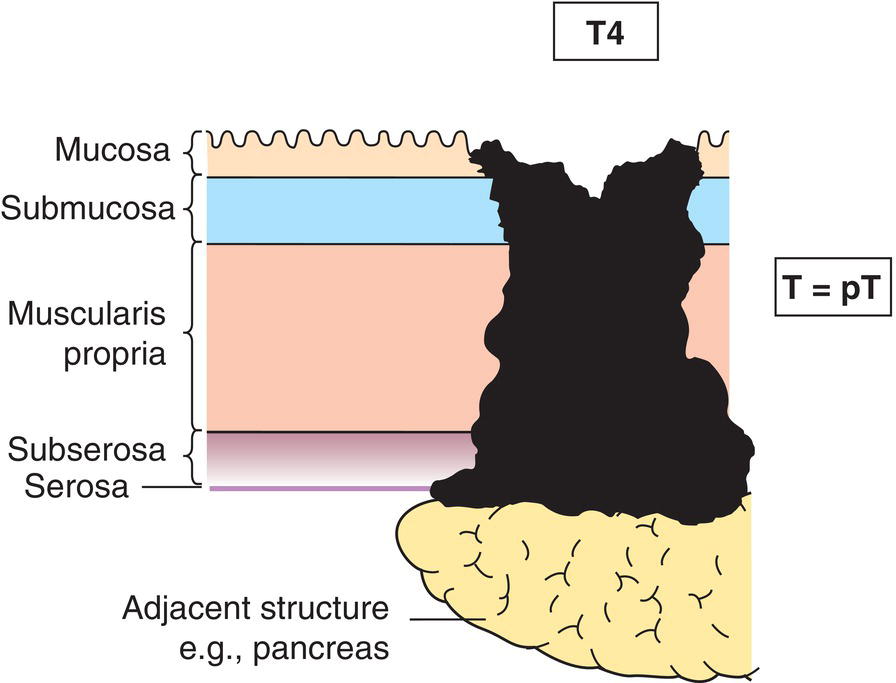
T4
Tumour perforates visceral peritoneum (serosa) (Fig. 246) or other organs or adjacent structures (Fig. 247) 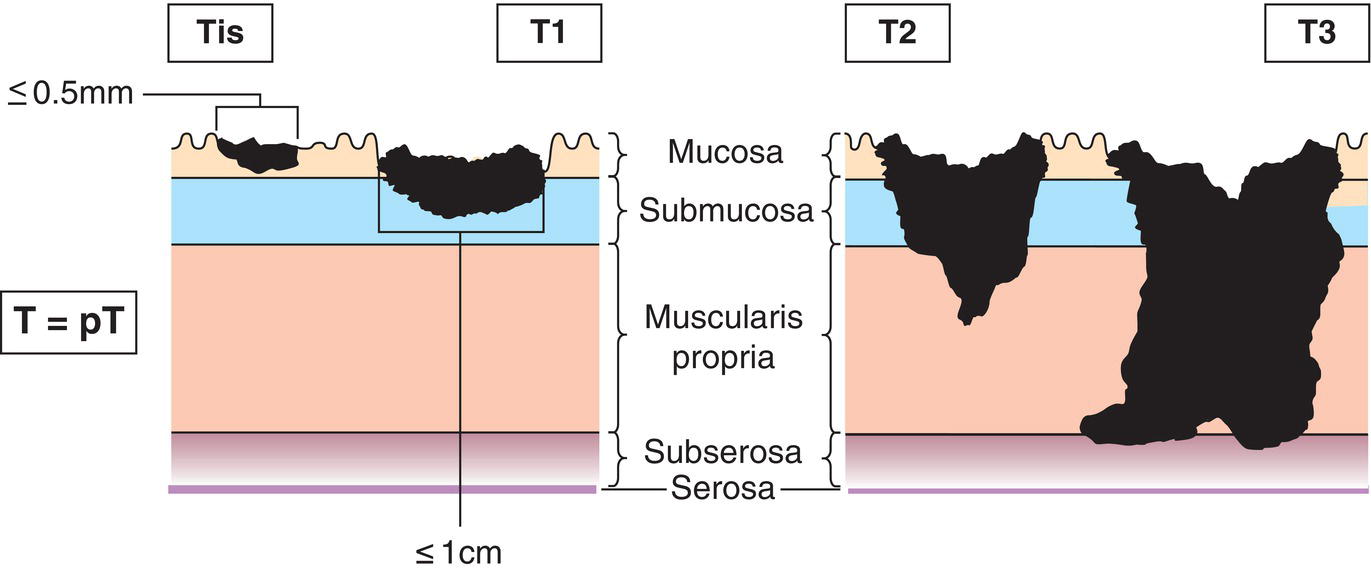
N – Regional Lymph Nodes
NX
Regional lymph nodes cannot be assessed
N0
No regional lymph node metastasis
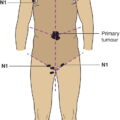
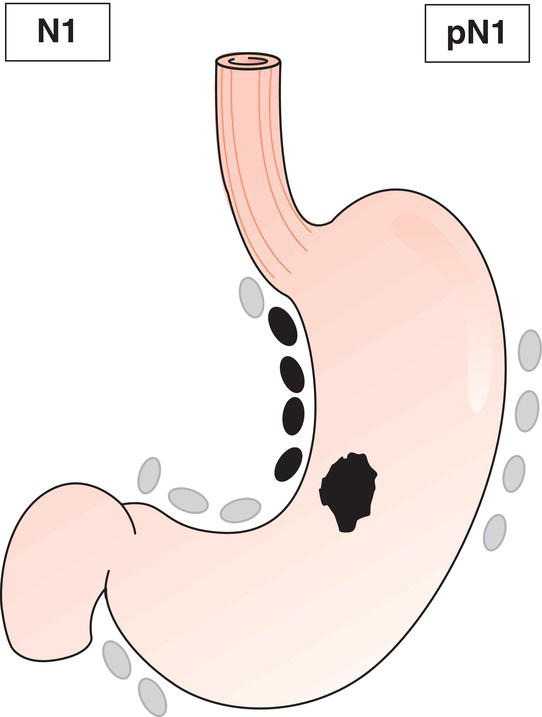
N1
Regional lymph node metastasis (Fig. 248)
M – Distant Metastasis
M0
No distant metastasis
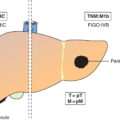
M1
Distant metastasis
M1a
Hepatic metastasis(es) only
M1b
Extrahepatic metastasis(es) only
M1c
Hepatic and extrahepatic metastases
Duodenum, Ampulla, Jejunum, Ileum
TNM Clinical Classification
T – Primary Tumour
TX
Primary tumour cannot be assessed
T0
No evidence of primary tumour
T1
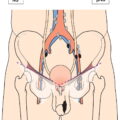
Ampullary: Tumour 1 cm or less in greatest dimension and confined within the sphincter of Oddi
Duodenal, Jejunum and Ileum: Tumour invades mucosa or submucosa and 1 cm or less in greatest dimension (Fig. 249)
T2
Ampullary: Tumour invades through sphincter into duodenal submucosa or muscularis propria, or more than 1 cm in greatest dimension (Fig. 249)
Duodenal, Jejunum and Ileum
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access