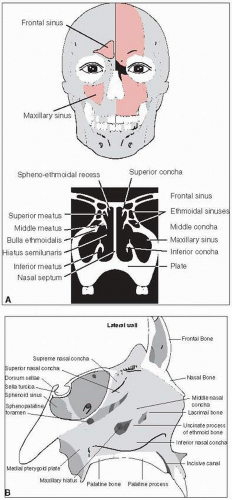
Nasal cavity and paranasal sinus cancers are twice as common in males as in females, and show a bimodal age distribution (10 to 20 and 50 to 60 years of age) (Fig. 15-1).
NATURAL HISTORY
Most lesions are advanced, and commonly involve the nasal cavity, several adjacent sinuses, and often, the nasopharynx.
There is often orbital invasion from maxillary sinus or ethmoid sinus cancers. Orbital invasion from nasal cavity tumors occurs later.
The anterior cranial fossa is invaded by way of the cribriform plate and roof of the ethmoid sinuses. The middle cranial fossa is invaded by way of the infratemporal fossa, pterygoid plates, or lateral extension from the sphenoid sinus.
Lesions involving the olfactory region tend to destroy the septum and may invade the nasal bone, producing expansion of the nasal bridge and, eventually, skin invasion.
Lesions of the anterolateral infrastructure of the maxillary sinus commonly extend through the lateral inferior wall and appear in the oral cavity, where they erode through the maxillary gingiva or the gingivobuccal sulcus. Tumors that extend posteriorly from the maxillary sinus have immediate access to the base of the skull.
Lymph node metastases generally do not occur until the tumor has extended to areas that contain abundant capillary lymphatics. The submandibular and the subdigastric lymph nodes are most commonly involved.
Nasal Vestibule
Lymph node spread from vestibule cancer is usually to a solitary ipsilateral submandibular or facial node, although bilateral spread occasionally is seen.
The preauricular and the submental nodes are at small risk.
Approximately 5% of patients have clinically positive lymph nodes on initial presentation; lymph node metastases develop in another 15% of patients after treatment has controlled the primary tumor (8).
DIAGNOSTIC WORKUP AND STAGING
A complete history and physical examination, including bimanual examination and cranial nerve assessment, is important in the workup. Fiberoptic nasal endoscopy may aid in evaluation of extent of disease.
CT scan is superior in detecting bone erosion or cribriform plate involvement, whereas T2-weighted MRI is more useful in differentiating between tumor and benign secretions. MRI is also useful in demonstrating intracranial, perineural, or leptomeningeal disease.
A chest x-ray, complete blood count, dental evaluation, and ophthalmologic examination should be performed to complete the pretreatment evaluation.
The American Joint Committee on Cancer staging system (2) groups nasal cavity and ethmoid sinus tumors together. A separate staging system applies to maxillary sinus tumors (Table 15-1). Nasal vestibule tumors are often staged using the system for skin cancer (see Table 9-1) (4).
FIGURE 15-1 Anatomy of nasal cavity and surrounding structures. A: Placement in skull, and cross section of nasal structures. B: Enlarged lateral view.
TABLE 15-1 American Joint Committee on Cancer TNM Classification for Cancer of the Nasal Cavity and Paranasal Sinuses
Primary Tumor (T)
Tx
Primary tumor cannot be assessed
TO
No evidence of primary tumor
Tis
Carcinoma in situ
Maxillary Sinus
T1
Tumor limited to maxillary sinus mucosa with no erosion or destruction of bone
T2
Tumor causing bone erosion or destruction including extension into the hard palate and/or middle nasal meatus, except extension to posterior wall of maxillary sinus and pterygoid plates
T3
Tumor invades any of the following: bone of the posterior wall of maxillary sinus, subcutaneous tissues, floor or medial wall of orbit, pterygoid fossa, ethmoid sinuses
T4a
Moderately advanced local disease. Tumor invades anterior orbital contents, skin of cheek, pterygoid plates, infratemporal fossa, cribriform plate, sphenoid or frontal sinuses
T4b
Very advanced local disease. Tumor invades any of the following: orbital apex, dura, brain, middle cranial fossa, cranial nerves other than maxillary division of trigeminal nerve (V2), nasopharynx, or clivus
Nasal Cavity and Ethmoid Sinus
T1
Tumor restricted to any one subsite, with or without bony invasion
T2
Tumor invading two subsites in a single region or extending to involve an adjacent region within the nasoethmoidal complex, with or without bony invasion
T3
Tumor extends to invade the medial wall or floor of the orbit, maxillary sinus, palate, or cribriform plate
T4a
Moderately advanced local disease. Tumor invades any of the following: anterior orbital contents, skin of nose or cheek, minimal extension to anterior cranial fossa, pterygoid plates, sphenoid or frontal sinuses
T4b
Very advanced local disease. Tumor invades any of the following: orbital apex, dura, brain, middle cranial fossa, cranial nerves other than (V2), nasopharynx, or clivus
Regional Lymph Nodes (N)
NX
Regional lymph nodes cannot be assessed
NO
No regional lymph node metastasis
N1
Metastasis in a single ipsilateral lymph node, 3 cm or less in greatest dimension
N2
Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm in greatest dimension, or in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension, or in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension
N2a
Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm in greatest dimension
N2b
Metastasis in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension
N2c
Metastasis in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension
N3
Metastasis in a lymph node, more than 6 cm in greatest dimension
Distant Metastasis (M)
MO
No distant metastasis (no pathologic MO; use clinical M to complete stage group)
M1
Distant metastasis
Stage Grouping
Stage 0
Tis
NO
MO
Stage I
T1
NO
MO
Stage II
T2
N1
MO
Stage III
T1
N1
MO
T2
N1
MO
T3
NO
MO
T3
N1
MO
Stage IVA
T4a
NO
MO
T4a
N1
MO
T4a
N2
MO
T1
N2
MO
T2
N2
MO
Only gold members can continue reading. Log In or Register to continue