The clinical presentation of pheochromocytoma has changed dramatically since Dr. Charlie Mayo successfully resected the first pheochromocytoma in North America in 1926. In the early days nearly all patients presented with hypertension and signs and symptoms of catecholamine excess. However, at Mayo Clinic since 2005, in most patients with pheochromocytoma their tumor was discovered incidentally on imaging performed for other reasons. We have also learned over the past two decades that although all pheochromocytomas have malignant potential, they grow slowly over time—by approximately 3–5 mm in diameter per year. Herein we share such a case.
Case Report
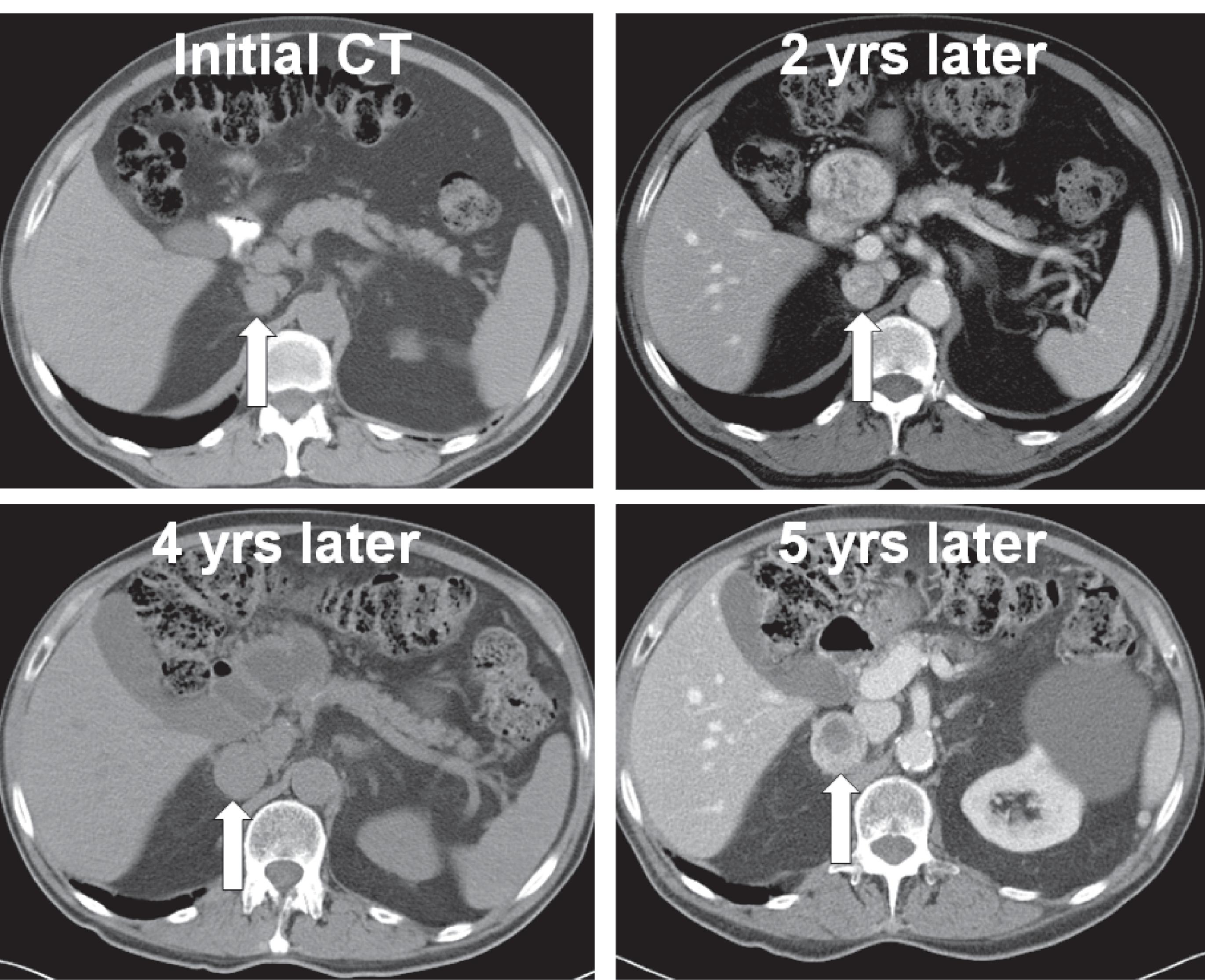
The patient was a 71-year-old man referred for evaluation of an incidentally discovered right adrenal mass. The initial computed tomography (CT) scan was obtained 5 years previously to evaluate left lower quadrant abdominal pain and incidentally detected a 1.8-cm right adrenal mass that was lipid poor (40.6 Hounsfield units [HU]) on unenhanced images ( Fig. 35.1 ). Subsequent CT scans demonstrated that the right adrenal mass was enlarging by an average of 4 mm in diameter per year and at the time of referral to endocrinology measured 3.8 × 3.3 cm (see Fig. 35.1 ). The patient was asymptomatic. His hypertension of 5 years duration was effectively treated with a calcium channel blocker (diltiazem 240 mg daily), an angiotensin receptor blocker (losartan 50 mg daily), and a β-adrenergic receptor blocker (metoprolol 25 mg daily). His diabetes of 2 years duration was treated with metformin (1000 mg twice daily) and rosiglitazone (4 mg twice daily). The patient had no signs or symptoms of adrenocortical or medullary dysfunction. He did have a history of prostate cancer treated with radiation therapy 3 years previously. His body mass index was 22.7 kg/m 2 , blood pressure was 120/70 mmHg, and heart rate 56 beats per minute.
INVESTIGATIONS
The laboratory studies were remarkable for marked elevation of normetanephrine in the blood and marked elevations of norepinephrine and normetanephrine the 24-hour urine collection ( Table 35.1 ). The patient was taking no medications that would cause false-positive elevations in norepinephrine or normetanephrine.
Related posts:
 45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
 Adrenocortical Carcinoma Associated With Lynch Syndrome
Adrenocortical Carcinoma Associated With Lynch Syndrome
 Cryoablation Therapy for Metastatic Paraganglioma
Cryoablation Therapy for Metastatic Paraganglioma
 Cushing Syndrome in the Setting of Multiple Endocrine Neoplasia Type 1
Cushing Syndrome in the Setting of Multiple Endocrine Neoplasia Type 1
 A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
 Catecholamine-Secreting Paraganglioma in Pregnancy
Catecholamine-Secreting Paraganglioma in Pregnancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


