Lymph Node Dissection or Systematic Lymph Node Sampling in the Chest
with care taken to avoid any hiatal hernias and preserve the vagus nerve in its medial location to the aorta.
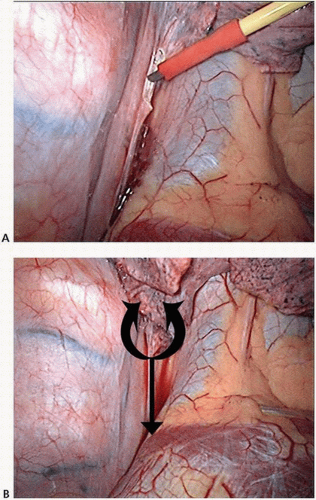 FIGURE 8-1 A,B: Thoracoscopic view of right-sided nodal dissection for stations 8 and 9. (Courtesy of Khalid Amer, FRCS [CTh].) |
impunity. (If diathermy is used, cutting these branches usually induces a cough reflex.) The bronchus intermedius and right main bronchus are identified and dissected proximally until the left main bronchus is identified. The subcarinal nodes are lifted off the pericardium (usually an avascular plane) and then dissected from their blood supply, with care taken to avoid injury to the membranous bronchus or esophagus (Fig. 8-4).
The nodes should be carefully labeled, as paraesophageal 8R and parabronchial 10R nodes could easily be mistaken for 7R nodes. In this location, injury to the thoracic duct is prevented by tucking the duct under the esophagus; lifting the esophagus off the vertebral bed may injure the thoracic duct. At the completion of this dissection, the right main bronchus, left main bronchus, and subcarinal space should be readily visible (Fig. 8-5).
 FIGURE 8-2 Exposure of station 8R by right thoracoscopy. IVC, inferior vena cava. (Courtesy of Khalid Amer, FRCS [CTh].) |
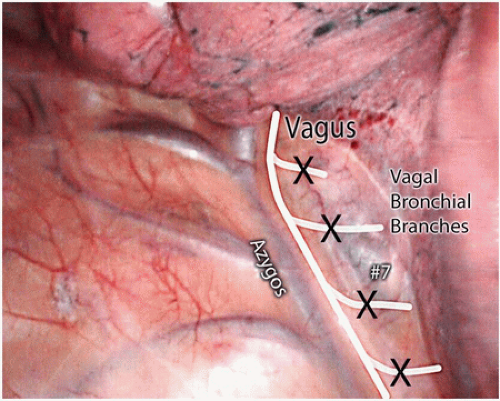 FIGURE 8-3 Right lung retracted forward to expose subcarinal nodes (level 7) via VATS approach. Small vagal branches towards lung can be divided without concern. (Courtesy of Khalid Amer, FRCS [CTh].) |
 FIGURE 8-4 Mobilization of the subcarinal nodal packet via the right chest. The pericardium is the anterior border of the dissection plane. (Courtesy of Khalid Amer, FRCS [CTh].) |
 FIGURE 8-5 View of the subcarinal space after complete nodal dissection. (Courtesy of Khalid Amer, FRCS [CTh].) |
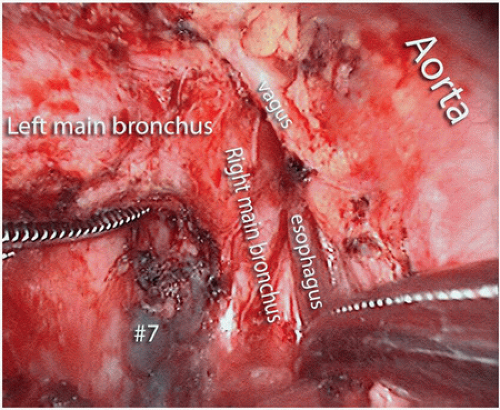 FIGURE 8-6 Subcarinal node dissection from the left chest. (Courtesy of Khalid Amer, FRCS [CTh].) |
a vessel loop is passed around the artery to facilitate its retraction. Gentle retraction of the carina in a downward direction and the artery in a cephalad direction exposes station 4L.
 FIGURE 8-7 View of the right upper mediastinum with anatomical boundaries of paratracheal node dissection. (Courtesy of Khalid Amer, FRCS [CTh].) |
the main pulmonary artery into the aortopulmonary space, medial to the vagus nerve (Fig. 8-10). The phrenic nerve is identified on the most medial aspect of the triangle. The nodal block is dissected up to the origin of the left subclavian artery, and all nodes and fatty tissue superficial to the ligamentum are harvested. As long as the dissection is kept to the medial side of the vagus, the recurrent laryngeal nerve is free from potential injury.
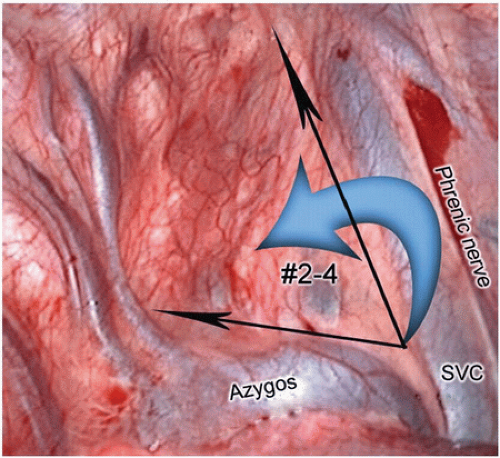 FIGURE 8-8 Black arrows indicate ideal sites for incising the mediastinal pleura, then performing an anterior to posterior mobilization of all soft tissue (blue arrow), including nodes behind the superior vena cava towards the vagus nerve. (Courtesy of Khalid Amer, FRCS [CTh].) |
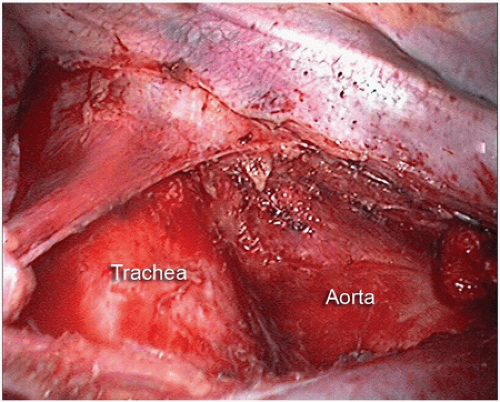 FIGURE 8-9 Right paratracheal node dissection basin after removal of all 2R and 4R nodal tissue. (Courtesy of Khalid Amer, FRCS [CTh].) |
 FIGURE 8-10 Exposure of level 5 (aortopulmonary window) nodes from behind the left hilum. (Courtesy of Khalid Amer, FRCS [CTh].) |
TABLE 8-1 Structures Dissected/Divided | ||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


