The prognosis of adrenocortical carcinoma (ACC) depends on several factors, including the European Network for the Study of Adrenal Tumours (ENSAT) stage, R0 (complete) surgical resection by an expert surgeon, and Ki-67 index. , Therapy with adjuvant mitotane, an adrenolytic agent, is usually recommended for patients at high risk of recurrence, such as ENSAT stage III disease. , Careful discussion of mitotane-associated side effects and monitoring should be performed before initiation of therapy.
Case Report
The patient was a 29-year-old man who developed an acute-onset severe abdominal pain in the right upper quadrant during jogging. He presented to a local emergency department where a computed tomography (CT) scan was obtained, and a right large adrenal mass was found. He was referred to our institution for further evaluation and management.
History was positive for nocturnal night sweats for several month but no other symptoms. His weightwas stable. On physical examination, his blood pressure was 136/97 mmHg and body mass index was 22 kg/m 2 . There was no evidence of any features of Cushing syndrome. He did not take any medications.
INVESTIGATIONS
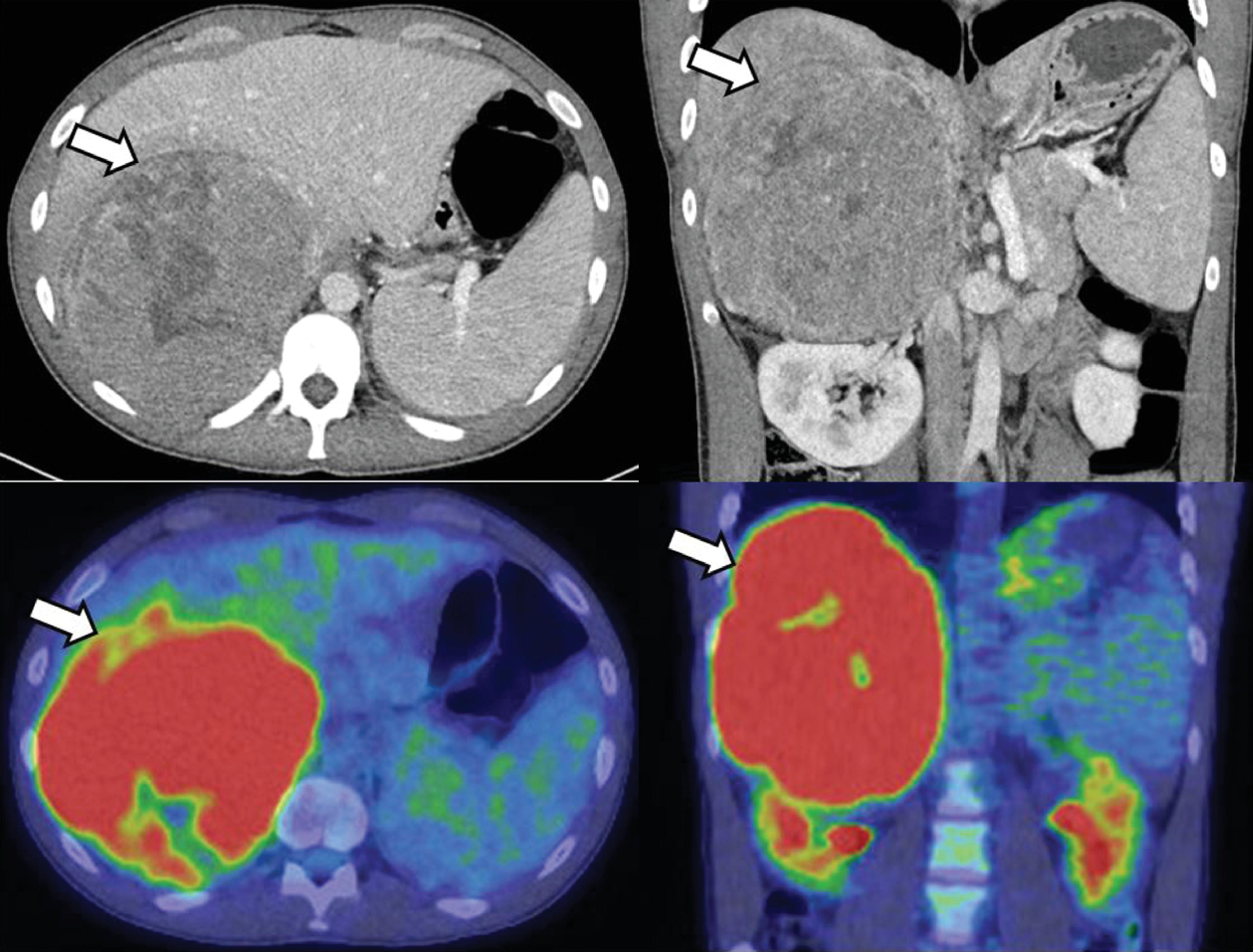
A large heterogeneous right adrenal mass measuring 14.6 × 14.0 × 17.0 cm with areas of internal calcification and central necrosis was demonstrated on CT scan ( Fig. 34.1 , upper panel). The mass caused inferior displacement of the right kidney, superior displacement of the liver, and compression of the inferior vena cava. Subsequent F-18 fluorodeoxyglucose (FDG) positron emission tomography (PET) scan demonstrated intense FDG uptake in the adrenal mass (maximum standardized uptake value = 9.9) without any other foci of activity (see Fig. 34.1 , lower panel).
Laboratory evaluation documented corticotropin (ACTH)-independent hypercortisolism and a 100-fold elevation in 11-deoxycortisol ( Table 34.1 ).
| Biochemical Test | Result | Reference Range |
| Cortisol after overnight 1-mg DST, mcg/dL | 11 | <1.8 |
| Cortisol, mcg/dL | 11 | 7–21 |
| ACTH, pg/mL | <5 | 7.2–63 |
| DHEA-S, mcg/dL | 548 | 105–728 |
| Pregnenolone, ng/dL | 243 | 33–248 |
| 17-Hydroxypregnenolone, ng/dL | 178 | 55–455 |
| 17-Hydroxyprogesterone, ng/dL | 157 | <220 |
| 11-Deoxycortisol, ng/dL | 7270 | 10–79 |
| Aldosterone, ng/dL | <4 | <21 |
| Plasma renin activity, ng/mL per hour | <0.6 | ≤0.6–3 |
| 24-Hour urine cortisol, mcg/24 h | 97 | <45 |
| Plasma metanephrine, nmol/L | <0.20 | <0.50 |
| Plasma normetanephrine, nmol/L | 0.24 | <0.90 |
TREATMENT
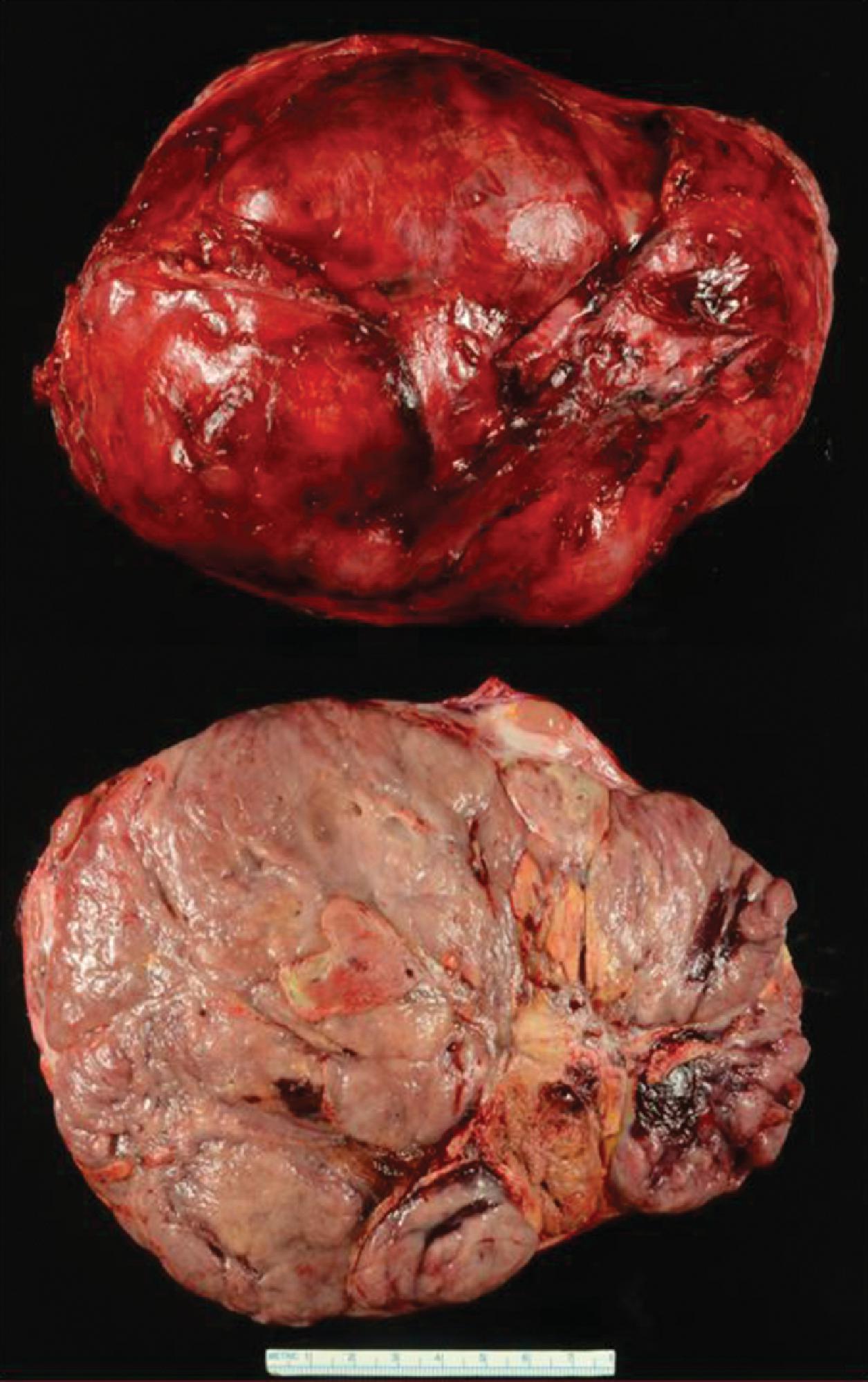
ACC was suspected because of concerning imaging characteristics, associated ACTH-independent hypercortisolism, and elevated 11-deoxycortisol. The patient was treated with open right adrenalectomy and segment 6 liver resection. The adrenal mass weighed 1865 g and measured 19.7 × 14.7 × 12.5 cm. The Ki-67 proliferation index was 15% ( Fig. 34.2 ). Although lymphovascular invasion was not identified, the tumor did invade through the adrenal capsule. Surgical margins were free of tumor. The patient was diagnosed with the ENSAT stage III disease. Postoperatively, 11-deoxycortisol decreased from 7270 ng/dL to 12 ng/dL (normal range, 10–79 ng/dL). He was initiated on hydrocortisone (20 mg daily in divided doses) treatment for anticipated adrenal insufficiency.
Related posts:
 45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
 Adrenocortical Carcinoma Associated With Lynch Syndrome
Adrenocortical Carcinoma Associated With Lynch Syndrome
 Cryoablation Therapy for Metastatic Paraganglioma
Cryoablation Therapy for Metastatic Paraganglioma
 Cushing Syndrome in the Setting of Multiple Endocrine Neoplasia Type 1
Cushing Syndrome in the Setting of Multiple Endocrine Neoplasia Type 1
 A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
 Catecholamine-Secreting Paraganglioma in Pregnancy
Catecholamine-Secreting Paraganglioma in Pregnancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


