MAGNESIUM DEFICIENCY
Part of “CHAPTER 68 – MAGNESIUM METABOLISM“
ETIOLOGY OF MAGNESIUM DEFICIENCY
Although magnesium is avidly conserved by the body, magnesium deficiency is a common occurrence. Up to 10% of the patients admitted to large city hospitals are hypomagnesemic.14 In one hospital, 65% of the patients in a medical intensive care unit were hypomagnesemic.15 Because magnesium is found in virtually all foods, dietary deprivation is a most unusual cause of hypomagnesemia in persons with normal caloric intake. Much more commonly, magnesium deficiency is caused by excessive losses from either the gastrointestinal tract or the kidney.16 Table 68-1 outlines causes of magnesium deficiency.
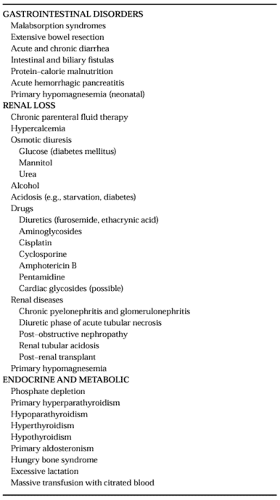 |
GASTROINTESTINAL DISORDERS
Magnesium may be lost via the gastrointestinal tract, either by excessive loss of secreted fluids or impaired absorption of both dietary and endogenous magnesium.2,7 The magnesium concentration of upper intestinal tract fluids is ˜0.5 mmol/L, and vomiting or nasogastric suction may contribute to magnesium depletion because of loss of these fluids. Disorders of the small bowel are frequently associated with magnesium deficiency.2,7 Intestinal mucosal damage from nontropical sprue, radiation injury from the treatment for Whipple disease, and intestinal lymphectasia may cause magnesium deficiency. Steatorrhea also may cause or potentiate magnesium malabsorption through formation of nonabsorbable magnesium-lipid salts. The resection or bypass of the ileum for obesity, enteritis, or vascular infarction often results in magnesium deficiency. The magnesium content of intestinal fluids can be as high as 15 mEq/L.17 Thus, excessive magnesium loss may occur in acute or chronic diarrheal states, including regional enteritis and ulcerative colitis, or in patients with intestinal or biliary fistulas. The diarrhea encountered in protein–calorie malnutrition may be one mechanism for magnesium depletion. Acute hemorrhagic or edematous pancreatitis can also produce hypomagnesemia. The reason is unclear, but it may be the result of saponification of magnesium in the necrotic peripancreatic fat, which is a mechanism similar to that proposed for the hypocalcemia of acute pancreatitis. A selective defect in intestinal magnesium absorption (primary intestinal hypomagnesemia) is thought to be one cause of neonatal hypomagnesemia.
RENAL LOSS
Urinary loss of magnesium is a common contributing cause of magnesium deficiency.2,13,18 The renal magnesium transport is influenced by the filtered sodium and calcium load. Thus, excess urinary excretion of sodium and calcium will increase magnesium clearance and lead to urinary magnesium losses. The administration of excessive sodium in parenteral fluids is a common factor in the pathogenesis of hypomagnesemia in hospitalized patients. Most disorders causing an increase in the serum calcium concentration will also lead to renal magnesium wasting, presumably because of activation of the Ca2+-sensing receptor in the thick ascending limb of Henle, resulting in a decrease in the transepithelial voltage and a subsequent decrease in calcium and magnesium reabsorption.11,19 An exception is familial hypocalciuric hypercalcemia caused by an inactivating mutation of the Ca2+-sensing receptor, and lithium ingestion, in which urinary magnesium excretion is decreased.
Commonly, diabetes mellitus is associated with magnesium deficiency and exemplifies osmotic-induced magnesium deficiency.20 The acidosis resulting from diabetic ketoacidosis, starvation, or alcoholism may also lead to renal magnesium wasting.2 The association of alcoholism with magnesium depletion is well known. Although the reason for magnesium deficiency is usually multifactorial in these patients, a rising blood alcohol level has been shown to cause renal magnesium loss.
A wide spectrum of therapeutic agents may be associated with renal magnesium wasting.21 Hypomagnesemia is observed with the use of loop diuretics, such as furosemide and ethacrynic acid, and with therapy with the aminoglycosides, cisplatin, cyclosporine, amphotericin B, and pentamidine.22 Cardiac glycosides increase renal magnesium loss in dogs, but the pathophysiologic role they play in human magnesium depletion is unclear.
Many renal glomerular and tubular diseases are associated with renal magnesium wasting.2 There may be other accompanying tubular abnormalities, and a reduced glomerular filtration rate (GFR) may or may not be present. A rare form of hypomagnesemia (primary renal hypomagnesemia) is characterized by renal magnesium wasting in the absence of any other renal abnormality. This disorder may occur in children or in adults and may be familial.
ENDOCRINE AND METABOLIC CAUSES
Other disorders may also be associated with a disturbance in magnesium metabolism.2,23 Phosphate depletion, which is a common problem in hospitalized patients, causes renal magnesium wasting. An increase in urinary magnesium excretion and occasional hypomagnesemia is seen also in primary hyperpara-thyroidism, treated hypoparathyroidism, and hyperthyroidism.2,24 In these situations, hypercalciuria probably promotes the renal magnesium losses. In hypothyroidism, low intracellular magnesium content is found in association with high serum magnesium levels. A tendency to low serum magnesium concentrations in primary aldosteronism may be related to renal magnesium wasting resulting from volume expansion. Marked hypomagnesemia may occasionally accompany the “hungry bone syndrome,” which is a phase of rapid bone mineral accretion most commonly seen in patients with preexisting hyper-parathyroid bone disease who undergo successful neck surgery for hyperparathyroidism. Hypomagnesemia caused by excessive lactation is a rare occurrence. Massive transfusion with citrated blood may result in hypomagnesemia as well as hypocalcemia.
MANIFESTATIONS OF MAGNESIUM DEFICIENCY
SIGNS AND SYMPTOMS
Pure magnesium deficiency in the absence of hormonal, gastrointestinal, or other metabolic disorders is uncommon. Signs and symptoms of magnesium deficiency are shown in Table 68-2. Because magnesium deficiency is usually associated with other disease states, the signs and symptoms of the primary disease process may mask those of magnesium deficiency.25 Neuromuscular hyperirritability may be the most common presenting problem in magnesium-depleted patients.2,23,26 Latent tetany may be present and may be elicited by positive Chvostek and Trousseau signs. Some patients may have spontaneous carpopedal spasm. Generalized seizures have also been reported. These neurologic signs in part may be caused by coexisting hypocalcemia. However, tetany has also been documented in magnesium-deficient patients with normal serum calcium levels.27 Other neurologic findings in hypomagnesemia include
athetoid and choreiform movements, nystagmus, ataxia, and vertigo. Psychiatric abnormalities have been reported. Muscular complaints, such as tremors, fasciculations, muscle wasting, and weakness, may also occur.
athetoid and choreiform movements, nystagmus, ataxia, and vertigo. Psychiatric abnormalities have been reported. Muscular complaints, such as tremors, fasciculations, muscle wasting, and weakness, may also occur.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


