CHAPTER 36 Lymphatic Filariasis
Lymphatic Filariasis at a Glance
Epidemiology
About 120 million people worldwide are infected with organisms causing lymphatic filariasis, 90% of them with W. bancrofti. B. timori occurs only on some small islands in Indonesia, and B. malayi is limited to Asia and several Pacific island groups including Indonesia and the Philippines. Infections due to W. bancrofti occur in sub-Saharan Africa, the Nile delta in Egypt and Sudan, south Asia, the western Pacific, and Central and South America, including islands in the Caribbean. The largest number of cases occurs in south Asia and tropical sub-Saharan Africa. Large-scale, aggressive control programs recently have decreased the prevalence of disease in many areas. Distribution of disease may be highly focal within affected areas (Fig. 36.1).

Fig. 36.1 Distribution of organisms causing lymphatic filariasis.
(Courtesy Nutman TB, Kazura JB. Filariasis. In: Guerrant RL, Walker DH, Weller PF, eds. Tropical Infectious Diseases, 2nd edn. Philadelphia: Churchill Livingstone; 2006:1154)
Etiology
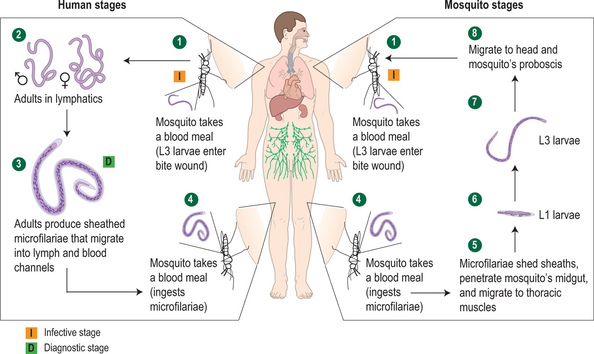
Larvae injected into the skin by the bite of the mosquito migrate to the lymphatics and develop into adult worms. Adult worms reside in the lymphatics and begin to produce microfilariae that are injected into the blood after 8 months in the case of W. bancrofti and 3 months in B. malayi.1 Adult worms may produce microfilariae for approximately 5–10 years, and microfilariae may live up to 1 year (Fig. 36.2). Microfilariae show a predominantly nocturnal periodicity, corresponding to the biting habits of the vector mosquitoes, though subperiodic strains are found in some geographical regions. Periodicity may also be influenced by the circadian rhythms of the human host.2
The prevalence of disease in a given area depends on a complex interaction of factors including intensity of transmission, genetic susceptibility, immunologic tolerance, prior treatment, and coinfections.3 Infection rates increase with age, representing the accumulation over a lifetime of adult-stage worms through continued exposure to infected vector mosquitoes. Frequency of disease manifestations also increases with age, though likelihood of developing clinical disease varies geographically. Overall, approximately one-third of those infected have some overt manifestations of disease.4
Clinical Manifestations
Asymptomatic filariasis
This group of infected individuals consists of those who have no overt disease manifestations and who may or may not have microfilaremia. Although disease may not be apparent, this may not be a completely clinically benign condition, as imaging techniques have revealed abnormalities of the structure and function of the lymphatics in affected individuals.5

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


