INTEGRATED APPROACH TO MANAGEMENT OF THYROID NODULES
Part of “CHAPTER 39 – THE THYROID NODULE“
The clinical challenge in thyroid nodule management is to define a diagnostic protocol that will produce the most accurate and cost-effective use of the various diagnostic methods. The implementation of decision analysis appears to highlight the difficulty in attaining this goal because consideration of all possible combinations of tests would require unmanageable decision trees, and the calculation of individual occurrence probabilities depends on an inconsistent literature. Limited decision analysis has suggested that FNA biopsy, the most accurate single evaluation technique, provides a minimal advantage in quality-adjusted life expectancy over the use of the usually inexact trial of thyroid suppression in patients already known to have solid, cold thyroid nodules. Either of these latter approaches appears slightly superior to a decision tree selecting immediate surgery when life expectancy is used as the gauge, but the differences may not be significant.7 On the other hand, analysis of the selection of radionuclide scanning indicates questionable benefit because initial aspiration can provide equal sensitivity and specificity at a lower cost.3,4,6,69
Figure 39-3 suggests an algorithm that may be useful in a practice in which FNA biopsy is frequently used and experienced cytopathologic support is available. Many factors may alter the protocol for individual patients or clinical practice situations. At present, no right or wrong approach exists, and many physicians prefer radionuclide imaging as the initial step. However, this may increase costs because only 5% to 10% of scans obviate the need for aspiration, whereas 60% of 80% of FNA biopsies eliminate scan requirements. The use of scans in identifying multinodularity is largely negated by the high incidence of benign cytology results in these cases. Aspiration and biopsy identify predominantly cystic lesions, which rarely are simple cysts; therefore, ultrasonography has limited use initially but may be of significant value in monitoring the results of suppressive therapy, especially in patients with suspicious lesions and in practices in which the patient may see different clinicians on follow-up. The argument can be made that the 20% to 25% cancer risk in suspicious lesions should lead to immediate surgery in all cases, but a trial of suppressive therapy may still be warranted in selected patients. In many borderline clinical situations, the patient’s strong preference or surgical risk factors may be important considerations. When a trial of suppressive therapy is undertaken, the approximate dosage required is >1.7 μg/kg per day of T4.81 The dose is increased incrementally by 0.025 mg per day every 5 to 6 weeks with TSH monitoring until TSH levels are reduced to the desired range. Usually the degree of TSH suppression need not be to an undetectable level but rather to a level of 0.1 to 0.3 mU/L. This should be the case particularly in postmenopausal women, in whom possible adverse effects of a fully suppressive dosage on bone mineral density are to be avoided. Nodules are assessed for change in size by physical examination (or ultra-sonography if required) every 6 weeks for the first 6 months. The follow-up intervals may be more prolonged when significant decreases in size are observed, extending eventually to annual follow-up.
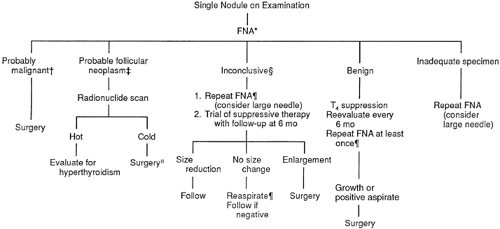 FIGURE 39-3. Approach to the solitary nodule. *22- to 25-gauge needle, repeated with 18-gauge needle if fluid is obtained. †Evidence of carcinoma (papillary, medullary, poorly differentiated, follicular) or lymphoma. ‡For example, sheets of follicular cells. §For example, small groups of uniform follicular cells with little colloid.|| Selected patients with above-normal surgical risk or other extenuating circumstances may be followed closely with suppressive therapy. ¶Changes in cytologic findings redirect clinician to the appropriate arm of the algorithm. (FNA, fine-needle aspiration; T4, thyroxine.)
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|


