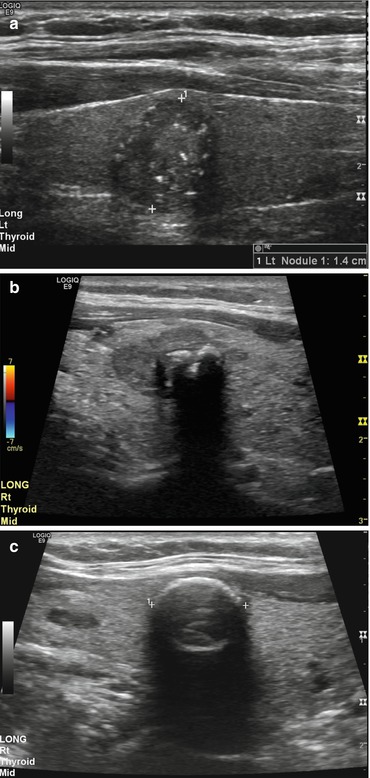
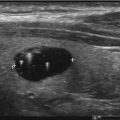
Fig. 5.1
Simple thyroid cyst

Fig. 5.2
Colloid cystic nodule
Another pattern to recognize as a benign nodule is the “spongiform nodule” also described in the literature as honeycomb or puff pastry appearance. All of these descriptors refer to the multiple small cystic spaces separated by thin septations which is shown in Fig. 5.3. These are considered highly likely benign and occur secondary to hyperplasia. Occasionally, bright echogenic foci may be found in these nodules. This finding needs to be closely interrogated, as the small cystic areas may have a bright linear interface at the posterior back wall of the cystic area which is benign and not to be confused with the malignant microcalcifications found within the stroma of a solid thyroid nodule.
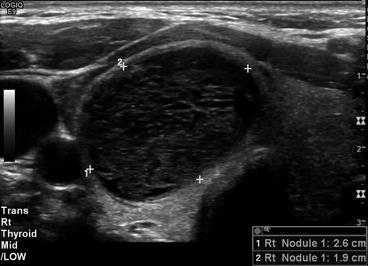
Fig. 5.3
Spongiform nodule
Another classic benign pattern is diffuse tiny hypoechoic nodules . Figure 5.4 demonstrates this classic appearance of Hashimoto’s thyroiditis also known as chronic lymphocytic thyroiditis. These nodules range in size from 1 to 6 mm which pathologically is related to a lymphoplasmacytic infiltrate and lymphoid follicles and may have intervening echogenic bands of tissue, which correspond to fibrosis pathologically. The gland is usually symmetrically involved. This appearance has a 95% positive predictive value for Hashimoto’s thyroiditis [1, 5]. Vascularity is not helpful as it may be normal, increased, or decreased. Nodules are also commonly associated with Hashimoto’s thyroiditis. Careful evaluation of each nodule is warranted as studies have shown an increased risk of papillary thyroid carcinoma around 16% as well as an association with primary thyroid lymphoma [6, 7]. Figure 5.5 demonstrates a widely accepted, but rarely seen, benign nodule pattern found in Hashimoto’s thyroiditis the giraffe pattern or giraffe hide. This is described as geographic areas of increased echogenicity which are bounded by thin intervening bands of hypoechogenicity similar to the color pattern seen on giraffes. The echogenic nodule seen in Fig. 5.6 is a variation of this benign process. Sometimes referred to as a “white knight,” this nodule pathologically represents a benign regenerative nodule of Hashimoto’s thyroiditis [2].There are also a few patterns associated with malignancy. The most common and well-known malignant pattern is that of a hypoechoic solid nodule with microcalcifications or punctate echogenic foci. This is shown in Fig. 5.7. The vast majority of papillary thyroid cancers are hypoechoic with a high sensitivity but low specificity as many benign nodules are also hypoechoic. Microcalcifications have a low sensitivity but high specificity. This has been shown in several meta-analyses [8, 9]. Combining these two features yields a combination that increases specificity for papillary thyroid carcinoma. The echogenic foci are secondary to tiny calcifications which may be psammoma bodies and/or amorphous calcium deposits. The psammoma bodies are likely secondary to necrotic cells causing calcium to laminate around this nidus. The amorphous calcifications may occur secondary to degeneration or fibrosis. Both are present in papillary thyroid carcinoma.
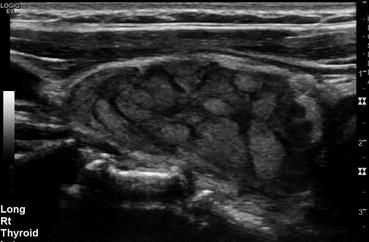
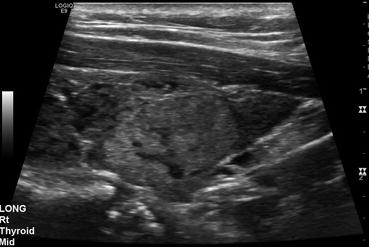
Fig. 5.4
Diffuse tiny hypoechoic nodule pattern
Fig. 5.5
Giraffe pattern
Fig. 5.6
Echogenic nodule
Fig. 5.7
Hypoechoic solid nodule with microcalcifications or punctate echogenic foci
Another pattern associated with malignancy is a hypoechoic solid nodule with coarse calcification centrally as seen in Fig. 5.8. This example demonstrates a well-demarcated rim of a hypoechoic nodule with central dense calcification felt to be suggestive of medullary carcinoma. [1] However, as medullary carcinoma accounts for only 3–5% of all thyroid carcinoma, macrocalcifications are more commonly seen in papillary carcinoma, and this is likely secondary to conglomeration of microcalcifications [10]. It is important to note that the coarse calcification is also common in benign nodules and multinodular goiter which is dystrophic in etiology. Therefore, this combination of a hypoechoic nodule with coarse calcification is the worrisome pattern, and coarse calcification alone is not worrisome on its own.
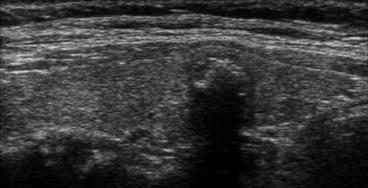
Fig. 5.8
Hypoechoic solid nodule with coarse calcification centrally
These patterns have been shown to be specific when present, but not sensitive enough to pick up all malignancies or stratify all nodules. Therefore, many groups have sought to implement classification schemes to include more appearances and characteristics which have been called thyroid imaging reporting and data systems (TI-RADS).
Thyroid Imaging Reporting and Data Systems
Multiple papers have been written on proposed TI-RADS . While there is no consensus statement on the use of these systems, many health systems are beginning to use variations. The primary impetus was to standardize thyroid nodule imaging and reports to yield dependable and reproducible malignancy risk stratification. These systems have been modeled after the Breast Imaging Reporting and Data System (BI-RADS) from the American College of Radiology (ACR). These vary from having specific descriptors fall into certain risk categories to assigning a point value to each description that are then added up to the sum that falls into a risk category. All of the proposed models use similar terminology for categorizing thyroid nodules using the numerical system or a risk descriptor For example, TI-RADS 1 is equivalent to normal/benign, TI-RADS 2 is equivalent to benign/probably benign, TI-RADS 3 is equivalent to probably benign/indeterminate, TI-RADS 4 is equivalent to suspicious/probably malignant, and TI-RADS 5 is equivalent to highly suggestive of malignancy [11, 12]. These categories have been divided differently in different studies but correspond to a risk of malignancy in the range of 0–2% in TI-RADS 1, 2–10% in TI-RADS 2, 2–30% in TI-RADS 3, 5–92% TI-RADS 4, and 80–100% in TI-RADS 5 [11, 12]. The ACR is expected to release TI-RADS within the next year after a meta-analysis of the many proposed systems already published. This should increase consistency across radiology departments. In 2015 the ACR expert committee started the process by producing a thyroid ultrasound reporting lexicon to begin standardizing the reporting process.
Thyroid Ultrasound Reporting Lexicon
The American College of Radiology (ACR) published a thyroid ultrasound reporting lexicon in 2015 [13]. This lexicon divides the reporting lexicon into six categories. A summary of these categories follows.
Category 1 is for composition. The recommended terminology includes cystic described as completely fluid filled, predominately cystic where the soft tissue component is less than 50% of the volume, predominately solid where the soft tissue component occupies greater the 50% of the volume, solid described as nearly completely solid with only a few tiny cystic spaces, and spongiform, which has been previously discussed in this chapter, composed of multiple tiny cystic spaces. Figure 5.9 demonstrates these five composition descriptors.
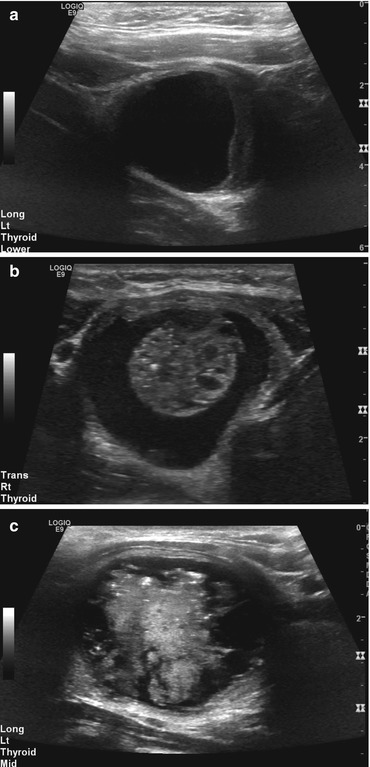
Fig. 5.9
Category 1: composition. (a) Cystic; (b) Predominately cystic; (c) Predominately solid; (d) Solid; (e) Spongiform
Category 2 provides four options for echogenicity, all of which are compared to surrounding tissue. Hyperechoic is increased compared to thyroid parenchyma, isoechoic is similar compared to thyroid parenchyma, hypoechoic is decreased compared to thyroid parenchyma, and very hypoechoic is decreased compared to neck musculature. Examples are demonstrated in Fig. 5.10. Category 3 is shape of the nodule, of which the only shape identified in several meta-analyses to have a significant sensitivity and specificity is taller than wide as seen in Fig. 5.11.
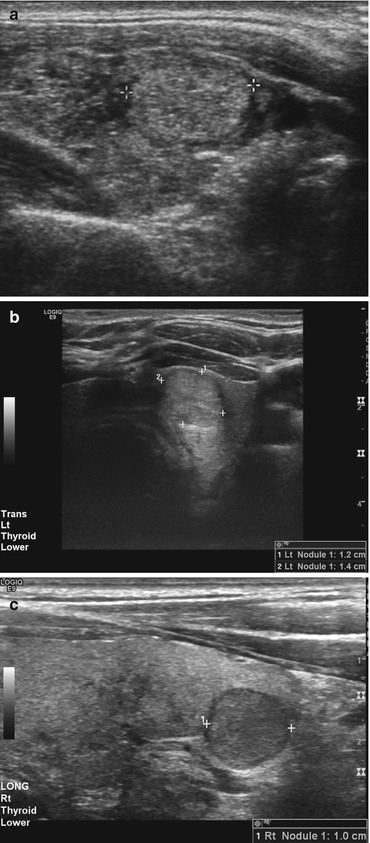

Fig. 5.10
Category 2: echogenicity. (a) Hyperechoic; (b) Isoechoic; (c) Hypoechoic; (d) Very hypoechoic
Fig. 5.11
Category 3: shape taller than wide
Category 4 is the size of the nodule. Thyroid nodules should be measured in three planes: longitudinal, transverse, and anteroposterior. Measuring is more important for follow-up comparison than a criterion to determine biopsy. Category 5 has six margin descriptions, all of which are demonstrated in Fig. 5.12. Smooth is found on spherical or elliptical nodules with a well-defined edge. Irregular describes spiculated, jagged, or sharp angles with protrusions into the surrounding parenchyma. Lobulated margins are rounded protrusions into the surrounding parenchyma. Ill-defined margins are those where it is not possible to clearly define the margin. Halos are a dark border at the periphery of the nodule and may be incomplete. The last margin descriptor is extrathyroidal extension where the nodule has broken through the thyroid capsule.
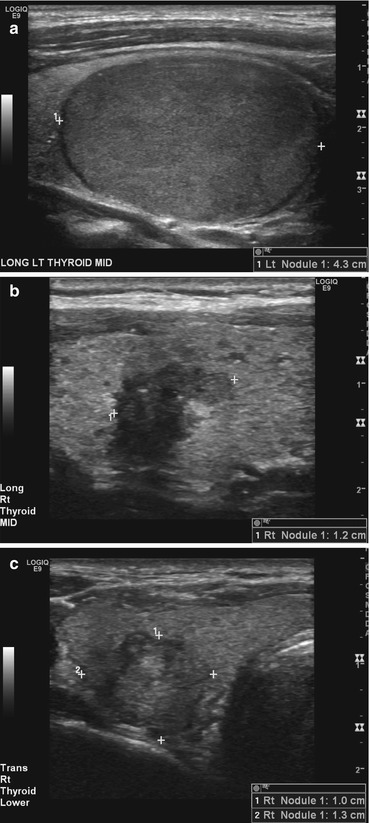
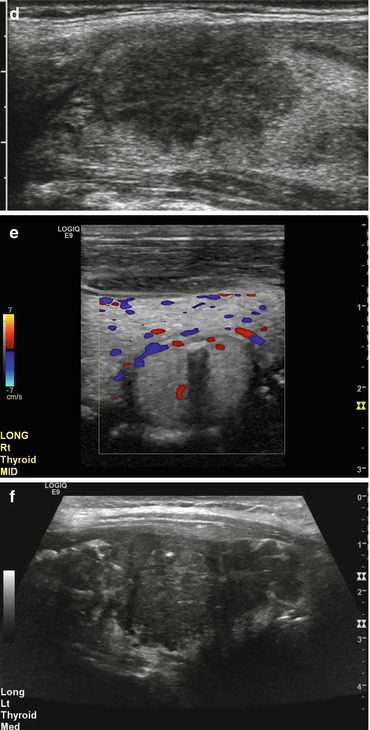
Fig. 5.12
Category 5: margin. (a) Smooth; (b) Irregular; (c) Lobulated; (d) Ill-defined; (e) Halo; (f) Extrathyroidal extension
Category 6 is echogenic foci. Punctate echogenic foci are “dot-like” and less than 1 mm. Macrocalcifications are large enough to generate a posterior acoustic shadow. Peripheral calcification encompasses the majority of the nodule. Comet tail artifacts are reverberation artifacts that are triangular in shape. Examples of these various types of echogenic foci are shown in Fig. 5.13 [13].