 |
CONGENITAL DISORDERS
Turner syndrome (Ullrich-Turner syndrome; gonadal dysgenesis) is a relatively common disorder with a frequency in the range of 1 in 1500 to 1 in 2500 female births.94 It is caused by an incomplete complement of X chromosomes, most commonly
secondary to the complete absence of one of the X chromosomes (45,XO). Partial deletions of the X chromosome or mosaicism with multiple cell lines, at least one of which is 45,XO, are less frequent etiologies. Occasionally, there may be smaller deletions of the long arm of the X chromosome that result in primary gonadal failure without other phenotypic features of the syndrome95; these deletions may not be seen on a routine karyotype. Girls with Turner syndrome have short stature that may be due to haploinsufficiency of the SHOX (short-stature homeobox-containing) gene, located in the pseudoautosomal region of the sex chromosomes.96 Other phenotypic features are variable in expression and include webbed neck, low posterior hairline, rotated ears, high arched palate, broad chest with the appearance of widely spaced nipples, increased carrying angle (cubitus valgus), short metacarpals, congenital lymphedema of the hands and feet, and dysplastic hyperconvex nails (Fig. 92-9).Congenital heart disease occurs in ˜25% of cases, with bicuspid aortic valve and aortic coarctation being most frequent. Renal anomalies and autoimmune thyroid disease are also frequent findings, occurring in more than one-third of girls.97
secondary to the complete absence of one of the X chromosomes (45,XO). Partial deletions of the X chromosome or mosaicism with multiple cell lines, at least one of which is 45,XO, are less frequent etiologies. Occasionally, there may be smaller deletions of the long arm of the X chromosome that result in primary gonadal failure without other phenotypic features of the syndrome95; these deletions may not be seen on a routine karyotype. Girls with Turner syndrome have short stature that may be due to haploinsufficiency of the SHOX (short-stature homeobox-containing) gene, located in the pseudoautosomal region of the sex chromosomes.96 Other phenotypic features are variable in expression and include webbed neck, low posterior hairline, rotated ears, high arched palate, broad chest with the appearance of widely spaced nipples, increased carrying angle (cubitus valgus), short metacarpals, congenital lymphedema of the hands and feet, and dysplastic hyperconvex nails (Fig. 92-9).Congenital heart disease occurs in ˜25% of cases, with bicuspid aortic valve and aortic coarctation being most frequent. Renal anomalies and autoimmune thyroid disease are also frequent findings, occurring in more than one-third of girls.97
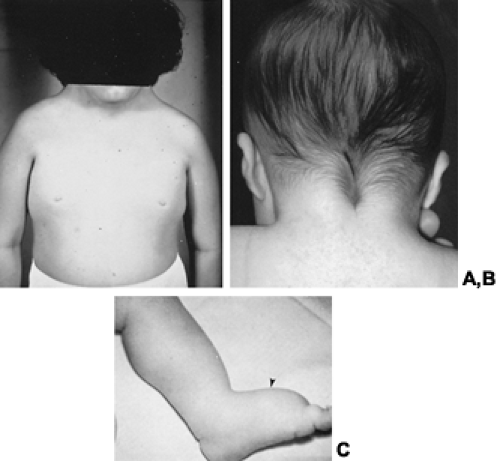 FIGURE 92-9. Turner syndrome. A,Webbed, short neck and broad, shield-like chest with the appearance of widely spaced nipples in a 10-year-old girl with Turner syndrome. Some features of Turner syndrome are obvious at birth and may include (B) low posterior hairline with tripartite appearance and (C) lymphedema of the extremities (arrowhead). |
As implied by its alternative name, gonadal dysgenesis, Turner syndrome is accompanied by primary gonadal failure in the majority of cases. This is due to a presumed acceleration of oocyte loss with a concomitant increase of stromal fibrosis, resulting in streak gonads.97 These processes are not inevitable, however, and some women with Turner syndrome, particularly those girls with mosaicism or partial X deletions, may have normal pubertal development and even achieve fertility. As demonstrated in one study, up to 16% of girls may have spontaneous puberty, including menarche.98 Gonadotropin levels are markedly elevated in a diphasic pattern (infancy to early childhood and after the age of 10 years) in girls with Turner syndrome.99 Levels of LH and FSH measured at these ages, therefore, may serve as helpful markers of impaired gonadal function, if elevated (see Chap. 90). Furthermore, pelvic ultrasonography to assess ovarian size and appearance has been advocated by some as a prognostic indicator of future pubertal development.100
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


