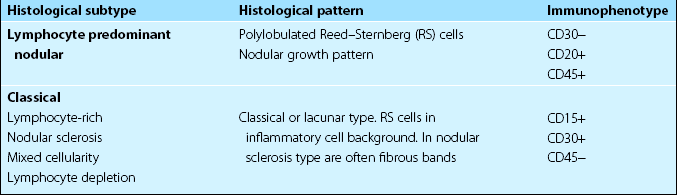
29 Hodgkin’s lymphoma is an unusual malignancy in that the malignant cells, termed Reed–Sternberg cells (Fig 29.1), and mononuclear Hodgkin’s cells form only a minority of the tumour. The remainder is composed of very variable numbers of other cells including lymphocytes, granulocytes, fibroblasts and plasma cells. This inflammatory cell infiltrate presumably reflects an immune response by the host against the malignant cells. Reed–Sternberg (RS) cells appear to originate from germinal-centre B-lymphocytes. In classical HL the RS cells are ‘crippled’ germinal-centre B-cells incapable of secreting immunoglobulins, while in lymphocyte predominant nodular HL RS cells the coding regions of the immunoglobulin genes are intact and potentially functional. Fig 29.1 Reed–Sternberg cells in a lymph node biopsy. It is acknowledged in the World Health Organization (WHO) classification (see also p. 60) that ‘Hodgkin’s disease’ comprises two distinct ‘Hodgkin’s lymphomas’ with different clinical features: classical HL and lymphocyte predominant nodular HL (Table 29.1). Asymmetrical and painless lymphadenopathy, most often in the cervical region, is the most common presentation. The nodes usually gradually enlarge but may fluctuate in size. Patterns of disease suggest contiguous spread via the lymphatic chain. Mediastinal involvement is a particular feature of the nodular sclerosing histological subtype (Fig 29.2). Splenomegaly and hepatomegaly occur but massive enlargement is rare.
Hodgkin’s lymphoma
Aetiology
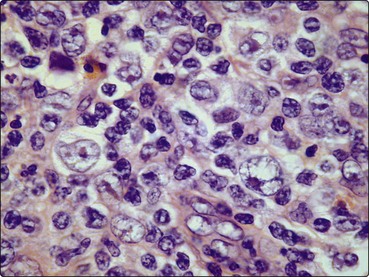
This giant cell is binucleated or multinucleated with large inclusion-like nucleoli and abundant cytoplasm.
Classification
Clinical presentation
Hodgkin’s lymphoma