properties of the HIT antibodies, which also generate procoagulant, platelet-derived microparticles45, 46; (b) pancellular activation (either directly or indirectly by HIT antibodies),47, 48 manifesting as tissue factor expression on endothelium25, 48, 49 and monocytes,50, 51 and possibly platelet-leukocyte complex formation52; and (c) neutralization of the heparin anticoagulant effects by PF4. Collectively, these factors result in increased thrombin generation in HIT.8, 53, 54
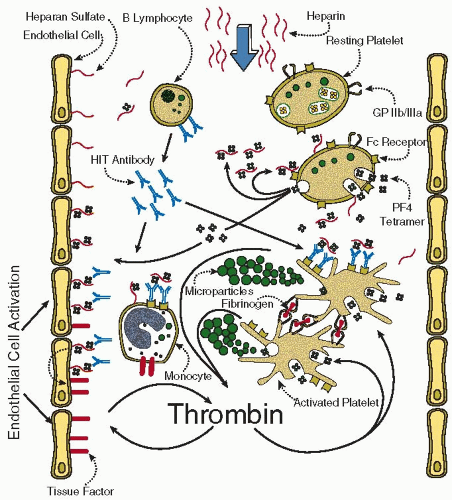 FIGURE 108.1 Pathogenesis of HIT. Heparin produces mild platelet activation, resulting in the release of PF4 from platelet α-granules and in the formation of immunogenic PF4/heparin complexes. B lymphocytes generate IgG that recognize the PF4/heparin complexes; the Fc “tails” of the IgG bind to platelet FcγII receptors, resulting in Fc receptor clustering and consequent strong platelet activation. Platelet aggregation is mediated by glycoprotein (GP) IIb/IIIa. Platelet-derived microparticles that accelerate thrombin generation are produced. The HIT antibodies also recognize PF4 bound to endothelial heparan sulfate, leading to tissue factor expression on endothelium. HIT antibodies also can activate monocytes. In all, increased thrombin generation results can explain some of the unusual clinical manifestations of HIT (e.g., venous limb gangrene and DIC) and provide a rationale for treatment that reduces thrombin generation. (From Greinacher A, Warkentin TE. Treatment of heparin-induced thrombocytopenia: an overview. In: Warkentin TE, Greinacher A, eds. Heparin-induced thrombocytopenia, 4th ed. New York: Informa Healthcare USA, 2007:283-317.) |
dose of anticoagulant in relation to surgery (postoperative > preoperative) and body mass index (BMI) (high BMI > low BMI).55, 62, 63, 64 A stoichiometric model of optimally immunizing PF4:heparin ratios has been proposed to explain some of these observations.64, 65
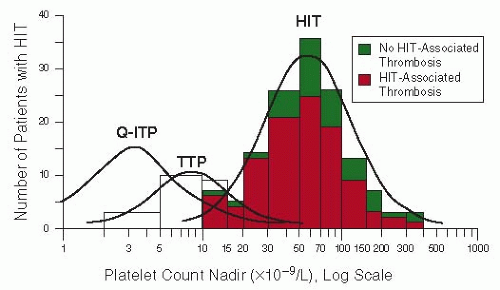 FIGURE 108.2 Platelet count nadirs in HIT, quinine-induced immune thrombocytopenic purpura (Q-ITP), and thrombotic thrombocytopenic purpura (TTP) with absent ADAMTS-13 activity. The majority of patients with HIT have HIT-associated thrombosis, and the risk of thrombosis is substantial irrespective of the severity of the thrombocytopenia. Data on TTP were kindly provided by James N. George, MD. (From Warkentin TE. Think of HIT. Hematology Am Soc Hematol Educ Program 2006:404-414, with permission.) |
count fall is rather uniform, for thrombotic events, the onset ranges widely, sometimes occurring even before the fall in platelet count is readily apparent, or up to several weeks later.14, 83, 88
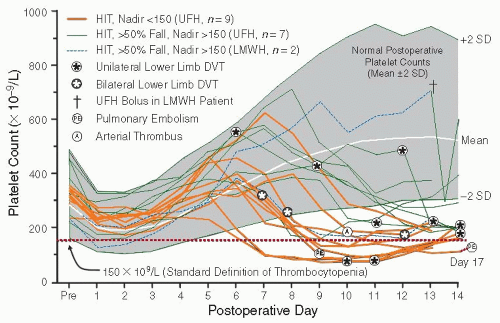 FIGURE 108.3 Characteristic timing, severity, and prothrombotic nature of HIT. The shaded area indicates the mean (±2 standard deviation [SD]) platelet count range in the reference population without HIT. There is an immediate postoperative decrease in the platelet count (maximal, days 1 to 3), followed by a rise to levels greater than baseline (maximal, days 11 to 14). Antithrombotic prophylaxis with subcutaneous UFH (7,500 U twice daily) or the LMWH, enoxaparin (30 mg twice daily), was begun usually on postoperative day 1. Eighteen patients developed HIT (50% or greater fall in the platelet count from the postoperative peak), with nine evincing a platelet count nadir <150 × 109/L and nine a platelet count nadir >150 × 109/L. The symbols indicate thrombotic events, 18 of which occurred in 13 of the 18 patients with HIT. One patient who received enoxaparin developed an abrupt platelet count fall when given a 5,000 U bolus of UFH (†). (Created from figures in Warkentin TE, Levine MN, Hirsh J, et al. Heparin-induced thrombocytopenia in patients treated with low-molecular-weight heparin or unfractionated heparin. N Engl J Med 1995;332:1330-1335; Warkentin TE, Roberts RS, Hirsh J, et al. An improved definition of immune heparin-induced thrombocytopenia in postoperative orthopedic patients. Arch Intern Med 2003;163:2518-2524.) |
Table 108.1 Complications of HIT | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
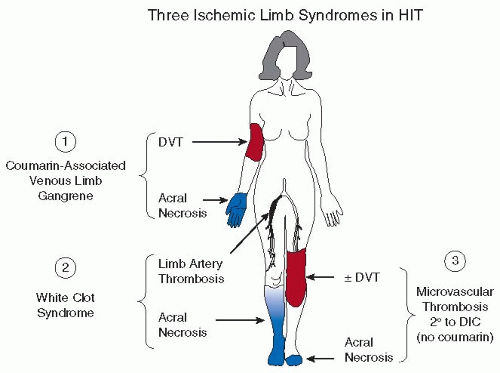 FIGURE 108.4 Three ischemic limb syndromes in HIT. The two most common causes of limb loss in HIT are coumarin-induced venous limb gangrene (microvascular thrombosis in a limb affected by DVT) and white clot syndrome (occlusion of large limb arteries by platelet-rich white clots). Rarely, microvascular thrombosis (with or without associated DVT) is associated with limb ischemia in the absence of coumarin use. DIC, disseminated intravascular coagulation. (Modified from Warkentin TE. Heparin-induced thrombocytopenia: IgG-mediated platelet activation, platelet microparticle generation, and altered procoagulant/anticoagulant balance in the pathogenesis of thrombosis and venous limb gangrene complicating heparin-induced thrombocytopenia. Transfus Med Rev 1996;10:249-258.) |
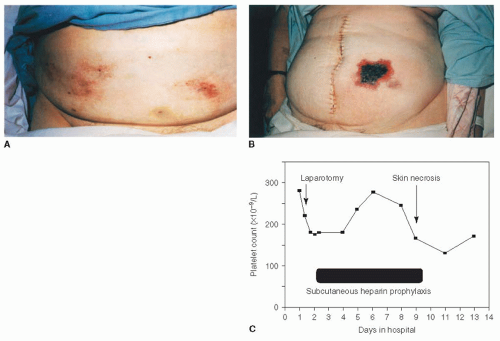 FIGURE 108.5 Heparin-induced skin necrosis. |
Table 108.2 Estimating the pretest probability of HIT: 4Ts scoring system | ||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||
Related posts:
 The Field of Hemostasis and Thrombosis: Selected Translational Achievements
The Field of Hemostasis and Thrombosis: Selected Translational Achievements
 Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
 Integrín αIIbβ3 and Platelet Aggregation
Integrín αIIbβ3 and Platelet Aggregation
 Inherited Thrombocytopenias
Inherited Thrombocytopenias
 Unusual Sites of Arterial Occlusion
Unusual Sites of Arterial Occlusion
 Blood Management in the Cardiovascular Surgical Patient
Blood Management in the Cardiovascular Surgical Patient
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


