Abstract
Normal menstrual cycling results from a complex and integrated process that requires the temporal coordination of hormonal secretion and signalling within the hypothalamic-pituitary-ovarian axis. Disruption of these signals at any point in the axis can manifest clinically as amenorrhea (the absence or abnormal cessation of menstrual cycles), or as oligomenorrhea (less than nine menstrual cycles a year). Primary amenorrhea refers to the failure to menstruate by age 15 years in the presence of normal secondary sexual development or within 5 years of breast development, if that occurs before age 10 years. Secondary amenorrhea refers to amenorrhea that occurs after menarche. The causes of oligomenorrhea and both primary and secondary amenorrhea are similar, and the differential diagnosis is extremely broad. Causes can be generally divided into genetic (covered here) and nongenetic. This chapter will therefore focus on genetic causes of oligomenorrhea that primarily affect ovarian and/or adrenal function. Specific attention will be given to the most common etiologies: primary ovarian insufficiency (POI), polycystic ovary syndrome (PCOS), and nonclassic congenital adrenal hyperplasia (CAH).
Keywords
amenorrhea, oligomenorrhea, nonclassic congenital adrenal hyperplasia, ovarian disorders, Turner’s syndrome, trisomy X, Down syndrome
Introduction
Normal menstrual cycling results from a complex and integrated process that requires the temporal coordination of hormonal secretion and signaling within the hypothalamic-pituitary-ovarian axis. Disruption of these signals at any point in the axis can manifest clinically as amenorrhea (the absence or abnormal cessation of menstrual cycles), or as oligomenorrhea (less than nine menstrual cycles a year). Primary amenorrhea refers to the failure to menstruate by age 15 years in the presence of normal secondary sexual development or within five years of breast development, if that occurs before age 10 years. Secondary amenorrhea refers to amenorrhea that occurs after menarche.
The causes of oligomenorrhea and both primary and secondary amenorrhea are similar, and the differential diagnosis is extremely broad. Causes can be generally divided into genetic (covered here) and nongenetic. The latter include psychosocial disorders (e.g., anorexia nervosa) as well as infectious, autoimmune, and metabolic conditions. Chromosomal and genetic causes are becoming increasingly appreciated as important and complex contributors to menstrual cycle abnormalities. Genetic disorders leading to defects in hypothalamic-pituitary regulation of the menstrual cycle, such as hypogonadotropic hypogonadism and Kallman’s syndrome, as well as mutations of the luteinizing hormone (LH) and follicle-stimulating hormone (FSH) receptors, are covered elsewhere in this book (see Chapter XX). This chapter will therefore focus on genetic causes of oligomenorrhea that primarily affect ovarian and/or adrenal function. Specific attention will be given to the most common etiologies: primary ovarian insufficiency (POI), polycystic ovary syndrome (PCOS), and nonclassic congenital adrenal hyperplasia (CAH).
Ovarian disorders
Primary Ovarian Insufficiency
POI refers to the cessation of ovarian function (i.e., ovulation and menstrual cycling) before the age of 40 years. The term primary ovarian insufficiency emphasizes that these disorders are intrinsic to the ovary and not the result of defects elsewhere in the hypothalamic-pituitary-ovarian axis. The diagnosis of POI is typically based on the presence of oligo- or amenorrhea in conjunction with circulating FSH levels that are in the menopausal range (usually above 40 IU/L) detected on at least two occasions a few weeks apart. The condition affects approximately 10–28% of women with primary amenorrhea and 4–18% of those with secondary amenorrhea. Although the majority of cases of POI are idiopathic, several familial cases have been identified. The overall prevalence of familial POI ranges from 4% to 31%. This wide range is likely due to variation regarding inclusion criteria and the detail sought in assessment of families. Pedigree analyses in affected families have identified global X-chromosome abnormalities, as well as specific mutations with autosomal dominant sex-linked inheritance or X-linked inheritance with incomplete penetrance.
Anti-Müllerian hormone (AMH) is produced by the granulosa cells of growing follicles and appears to inhibit the growth of primordial follicles. Clinically, serum AMH may be a useful biomarker of ovarian reserve. In women and mice, serum AMH declines with advancing age. Although it is difficult to establish a direct link between serum AMH and the primordial follicle pool in humans, antral follicle number is positively correlated with AMH levels.
X-Chromosome Abnormalities
Both familial and sporadic X-chromosome abnormalities have been described in women with POI. These include the complete absence of one X chromosome, as seen in Turner’s syndrome, trisomy X, as well as partial X-chromosome defects including deletions and balanced autosome translocations.
Turner’s Syndrome
Classic Turner’s syndrome is characterized by the absence of one X chromosome. Clinical features are variable, and at birth newborns may present with low birth weight, lymphedema of the upper and lower extremities (in 30% of Turner babies), and a webbed neck (pterygium colli). Additional dysmorphic features may include low-set prominent ears, a low posterior hairline, micrognathia, high-arched palate, epicanthal folds, hypoplastic nail beds, and/or hypoplastic fourth and fifth metacarpals. At adolescence, the most common presentation is one of short stature, amenorrhea, and lack of secondary sex characteristics, although the latter is variable and depends upon the extent of gonadal dysgenesis. The diagnosis of Turner’s syndrome should prompt a search for renal anomalies (incidence between 30% and 50%), as well as coarctation of the aorta and hearing loss.
Thirty percent of patients with Turner’s syndrome have the classic 45, X karyotype, and the remaining have a mosaic form where a 45, X cell line is associated with another cell line such as 46, XX or 46, XY. Of note, patients with mosaic forms of Turner’s syndrome can lack the classic phenotypic features, and usually are not diagnosed until presenting with POI later in life.
While one X chromosome in females is inactivated for dosage compensation, several genes escape inactivation and are essential for normal function of the X chromosome. The phenotypic traits of Turner’s syndrome, including POI, have been mapped to a critical region in Xp11.2-p22.1 which escapes X inactivation, and contains the 18 candidate genes that have been reported.
The loss of one X chromosome leads to an accelerated loss of ovarian follicles prior to birth. Many patients with Turner’s syndrome lose all of their follicles prenatally, and some lose their remaining germ cells during childhood. Accordingly, such patients will present with primary amenorrhea. Less than 15% of Turner’s patients will lose their germ cells after puberty and may even have enough germ cells for regular cycles before presenting with secondary amenorrhea. Rarely, some patients with Turner’s syndrome will even achieve pregnancy prior to developing ovarian insufficiency.
Once the germ cells are depleted from the ovaries, the residual gonads consisting only of connective stroma are called “streak gonads.” Patients with a Y cell line Turner’s syndrome have an increased risk of development of gonadoblastoma and malignant germ cell tumors. Consequently, it is recommended that streak gonads be surgically removed.
Trisomy X
Trisomy X affects one in 900 women and is rarely associated with POI. In one series, two of 52 (3.8%) patients with POI had trisomy X. The underlying mechanism is not clear, but may be similar to that observed among patients with Klinefelter’s syndrome.
Deletions
Deletions on an X chromosome leave a portion of the normal X unpaired and can lead to oocyte atresia. Although deletions more often involve the short arm of the X chromosome (Xp), deletions associated with POI more commonly involve the Xq13-25 region. Deletions at Xp11 result in both primary and secondary amenorrhea, whereas deletions at Xq13 usually lead to primary amenorrhea. It has also been noted that more proximal deletions are associated with ovarian failure while distal deletions appear to be innocuous. However, it remains unclear why large deletions that remove the whole critical region for POI, in Xq21, are not associated with ovarian failure.
Translocations
Balanced X/autosomal translocations, while rare, often lead to POI and have been reported in more than 100 postpubertal women. Breakpoints that fall between Xq13 and Xq26 are associated with ovarian failure. Thus, it has been proposed that this is a critical region for normal ovarian function. The most frequent breakpoints involve two specific POI regions: POI1 Xq26-qter, and POI2 Xq13.3-Xq21.1. The chromosome in this region may be particularly sensitive to structural changes that ultimately lead to oocyte apoptosis. Distal deletions involving the POI1 locus are typically associated with POI at age 24–39 years, whereas translocations involving the POI2 locus cause POI at an earlier age of 16–21 years.
POI Genes on the X Chromosome
Multiple candidate genes for POI have been proposed, although actual mutations have been identified in less than 10% of cases. Because the functions of many of these genes are not known, they are not used as genetic markers for POI.
Fragile X Metal Retardation ( FMR1 ) Gene
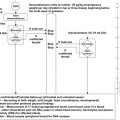
The most common form of inherited mental retardation, the fragile X syndrome, is associated with expansion of a CGG triplet repeat in the 5′ untranslated region of the FMR1 gene located in Xq27.3, outside the Xq POI critical region. Four types of alleles have been identified based on the number of repeats: normal (6–40), gray zone (41–60), premutated (61–200), and fully mutated (>200). The overall prevalence of the fragile X premutation ranges from 1/259 in a nonselected population of over 10,000 French-Canadian women to 1/100 in a population of Israeli women. Women who carry the fragile X premutation (61–200 repeats) are at risk for having a child with fragile X syndrome. In addition, the association between fragile X premutation carrier status and POI has been well documented. The results of an international study examining premature menopause in 760 women from families with fragile X syndrome showed that 16% of the 395 premutation carriers experienced menopause prior to the age of 40, compared with none of the 238 full mutation carriers and one (0.4%) of the 237 controls. Early menopause, however, is only one end of a spectrum of the ovarian dysfunction that occurs, since some women may have elevated serum FSH levels but maintain regular menstrual cycles. Collectively, premutation carriers experience earlier menopause by approximately 5 years.
The mechanism underlying the association between the fragile X premutation and POI, however, remains unclear. The FMR1 gene is expressed in oocytes and encodes an RNA-binding protein involved in translation. Few functional studies of the FMR1 protein have been performed with POI in view. Rather, theories are based on studies using neurons and lymphocytes from patients with a late-onset neurodegenerative disorder also associated with the fragile X premutation, termed fragile X tremor/ataxia syndrome. Premutation carriers are known to produce transcripts with large CGG repeat tracks. In the presence of the full fragile X mutation, however, the FMR1 gene is methylated, and its transcription is blocked. Since ovarian failure has not been demonstrated among women with the full mutation, it cannot be attributed to a lack of the FMR protein. Rather, it has been proposed that the large tracks of rCGGs act in a toxic manner through increased mRNA levels or the unusual structural features of the large repeat tracts in the transcripts. Such structures could bind other important proteins in the cell, rendering them inactive or targeting them for degradation. Alternatively, proteins or transcription factors that bind to the CGG repeats may be unable to perform their normal functions.
Since the fragile X premutation is one of the few genetic causes of premature ovarian failure that can be tested for, it is of particular importance to document the mutation for diagnostic purposes and for assessing the risk of bearing offspring of fragile X mental retardation.
In most people, the CGG segment is repeated in the gene approximately 5–44 times. Increased expression of the CGG segment on the FMR1 gene is associated with impaired cognitive and reproductive function.
Bone Morphogenetic Protein 15 Gene ( BMP15 )
Bone morphogenetic proteins (BMPs) are extracellular signaling proteins belonging to transforming growth factor-β superfamily that also includes growth/differentiation factors (GDFs) encoded by the BMP15 gene. BMP15 is an oocyte-specific GDF that stimulates folliculogenesis and granulosa cell growth and is expressed in oocytes during early folliculogenesis. It is thought that this protein may be involved in oocyte maturation and follicular development as a homodimer or by forming heterodimers with a related protein, Gdf9. The BMP15 gene is located within the POI critical region on Xp11.2.
In 2004, Di Pasquale et al. reported a heterozygous mutation in the BMP15 gene in two sisters with primary amenorrhea. The mutation involved an A to G transition at nucleotide 704 of the BMP15 gene produce Y235C. The father was unaffected as a hemizygous carrier and the mother had only wild-type BMP15 coding sequence. The mutation was not found in 210 alleles from 120 ethnically matched controls.
Autosomal Genes
Blepharophimosis-Ptosis-Epicanthus Inversus Syndrome (BPES)
BPES is an autosomal dominant condition characterized by eyelid malformations, low nasal bridge, and ptosis of the eyelids with (type I) or without (type II) POI. Both types map to 3q22-q23 and are associated with a mutation in the FOXL2 gene, which encodes a winged helix/forkhead transcription factor that plays an important role in development, present mostly in the craniofacial region, the pituitary gland, and ovary. Gene mutations leading to a truncated protein tend to produce BPES type I, whereas elongated proteins typically lead to BPES type II. In the human ovary, FOXL2 is expressed initially in cells of the female genital ridge prior to sex determination, and through adulthood is highly expressed in granulosa cells and to a lesser extent in theca and stromal cells. Ovarian failure may be caused by either a decreased number of follicles forming during development or an increased rate of follicle loss. In addition, since FOXL2 is also expressed during pituitary organogenesis, mutations that affect the hypothalamic-pituitary-gonadal axis may also play a role in ovarian failure.
Because the FOXL2 gene is the first human autosomal gene in which dominant mutations have been linked to ovarian function, its potential role in nonsyndromic POI has also been a subject of investigation. However, sequence analysis of the FOXL2 gene in a total of 290 nonsyndromic POI patients from five different studies found only one mutation potentially responsible for the POI. Thus, the role FOXL2 gene mutations in nonsyndromic POI remains unclear.
Inhibin ( INH ) Gene
Inhibin is a gonadal protein that inhibits the synthesis and secretion of FSH from the pituitary, and has been proposed as a strong candidate gene in POI. Low serum inhibin levels have been documented in women with POI. Inhibins have also been implicated in regulating numerous cellular processes including cell proliferation, apoptosis, and tumor suppressor activity. One variation of the INH alpha gene, G769A, has been associated with POI, the prevalence of which may vary in different populations from 0% to 11%.
Galactose-1-Phosphate Uridyltransferase ( GALT ) Gene
Galactosemia is a rare autosomal recessive disorder associated with an impairment in GALT metabolism and consequent excessive galactose levels. GALT deficiency is the most common type of galactosemia. Intracellular accumulation of galactose or its metabolites may cause follicular damage or decrease the number of oogonia formed initially, therefore leading to POI. The GALT gene maps to chromosome 9p13, and female patients with galactosemia have a 60–70% prevalence of POI. Women can present with primary amenorrhea, although the majority develop POI shortly after puberty.
Folliculogenesis Specific Basic Helix–Loop–Helix Gene Mutation ( FIGLA gene)
This gene encodes a protein that functions in postnatal oocyte-specific gene expression that regulates multiple oocyte-specific genes, including genes involved in folliculogenesis and those that encode the zona pellucida. Mutations in this gene cause POI. It seems likely that genetic hierarchies expressed within oocytes complement these somatic signals to maintain appropriate germ cell identity by activating oocyte-associated genes and repressing sperm-associated genes during postnatal oogenesis.
Zhao et al. analyzed the FIGLA gene in 100 Chinese women with POI and identified a 22-bp deletion ( 608697.0001 ) and a 3-bp in-frame deletion (140delN; 608697.0002 ) in two patients, respectively. The mutations were not found in 340 female controls with regular menstrual cycles and no history of infertility.
NOG Gene Mutations Causing Noggin Deficiency
Proximal symphalangism (SYM1) is an autosomal dominant disorder characterized by ankylosis of the proximal interphalangeal joint, fusion of the carpal and tarsal bones, brachydactyly, and conductive deafness. It is caused by haploinsufficiency of the NOG gene on 17q22 encoding Noggin. NOG is also expressed in the ovary and acts as an antagonist for bone morphogenic proteins (BMPs), including BMP 4 and BMP 7, which play an important role in ovarian function. POI has been reported in one female with SYM1 and a documented NOG gene, suggesting increase in the susceptibility to POI by disrupting the function of BMPs.
The Estrogen Receptor (ER)
The estrogen receptor (ER) exists primarily in two isoforms (ERalpha and ERbeta) with specific tissue and cell patterns of expression. The ER gene has been mapped to 6q25.1 and its product is a ligand-activated transcription factor. Variants in the ER have been associated with differences in the clinical expression of risk for breast carcinoma, bone mineral density (primarily in men), and age at menopause. In one large study of 900 postmenopausal women genetic variation in the ESR gene contributed to the variability in the onset of menopause. The ESR genotypes (PP, Pp, and pp) were assessed by polymerase chain reaction using the PvuII endonuclease to detect an anonymous intronic RFLP. Compared with women carrying the pp genotype, homozygous PP women had a 1.1 year ( P < 0.02) earlier onset of menopause. Furthermore, an allele dose effect was observed, corresponding to a 0.5 year ( P < 0.02) earlier onset of menopause per copy of the P allele.
Down Syndrome
Down syndrome is a genetic disorder caused by the presence of all or part of a third copy of chromosome 21 (Hsa21), which was first described in 1866. Depending on the maternal age structure of the population and the utilization of paternal testing, the incidence of trisomy 21 ranges from 1/600 to 1/1000 live births, making it one of the most common chromosomal abnormalities in live-born individuals. Like most trisomies, the incidence of trisomy 21 is highly correlated with maternal age, increasing from about 1/1500 live births for women 20 years of age to 1/30 for women ≥ 45 years.
Down syndrome is associated with intellectual disability, a characteristic facial appearance, and hypotonia. All affected individuals experience cognitive delays, but the intellectual disability is usually mild to moderate. Down syndrome is also associated with an increased risk of hypothyroidism (15%), core binding factor acute myeloid leukemia, and the development of Alzheimer disease. Approximately half of adults with Down syndrome develop Alzheimer disease, and they usually develop this condition in their fifties or sixties.
Most cases of Down syndrome result from trisomy 21; less commonly, Down syndrome occurs when part of chromosome 21 becomes translocated to another chromosome in a parent or very early in fetal development. A very small percentage of people with Down syndrome have an extra copy of chromosome 21 in only some cells (mosaic Down syndrome).
Most cases of Down syndrome are not inherited. When the condition is caused by trisomy 21, the chromosomal abnormality occurs as a random event during the formation of reproductive cells in a parent. Nondisjunction results in a reproductive cell with an abnormal number of chromosomes. If one of these atypical reproductive cells contributes to the genetic make-up of a child, the child will have an extra chromosome 21 in each of the body’s cells.
Individuals with translocation Down syndrome can inherit the condition from an unaffected parent. The parent carries a rearrangement of genetic material between chromosome 21 and another chromosome. This rearrangement is called a balanced translocation. No genetic material is gained or lost in a balanced translocation, so these chromosomal changes usually do not cause any health problems. However, as this translocation is passed to the next generation, it can become unbalanced. Individuals who inherit an unbalanced translocation-involving chromosome 21 may have extra genetic material from chromosome 21, which causes Down syndrome.
Early studies suggested that a limited region of Hsa21, termed the Down syndrome critical region (DSCR), might contain one or more dosage-sensitive genes that contribute to many of the Down syndrome phenotypes. However, further studies that included larger numbers of partial trisomy cases and more detailed genetic mapping have shown that different regions of Hsa21 contribute to different phenotypes, arguing against a single DSCR.
Polycystic Ovary Syndrome
In contrast to the relatively rare genetic disorders discussed above, polycystic ovary syndrome (PCOS) is among the most common hormonal disorders in women and accounts for a large majority of women presenting with menstrual irregularities. PCOS is characterized by irregular menstrual cycles and androgen excess, with symptoms typically emerging late in puberty or shortly following. After exclusion of other causes (hyperprolactinemia, nonclassic congenital adrenal hyperplasia (see below), Cushing’s syndrome) diagnosis requires at least two of the following to be present: oligoovulation or anovulation, typically presenting as oligomenorrhea or amenorrhea, hyperandrogenemia without or with clinical manifestations of androgen excess including acne, hirsutism, and/or hair thinning in a male pattern, and polycystic ovaries on ultrasonography. Although not included in the formal definition, PCOS is also associated with a variety of metabolic abnormalities including obesity, impaired glucose tolerance, type 2 diabetes, hyperlipidemia, and obstructive sleep apnea.
Multiple etiologic factors, at all levels of the hypothalamic-pituitary-ovarian axis, have been implicated in the pathogenesis of PCOS that ultimately lead to increased ovarian androgen biosynthesis. For instance, there is an increased frequency of hypothalamic gonadotropin-releasing hormone (GnRH) pulses that favor the production of LH over FSH. The relative increase in pituitary secretion of LH leads to an increase in androgen production by ovarian theca cells.
Insulin also plays an important role in the pathogenesis of PCOS by acting synergistically with LH to enhance androgen production by theca cells. In addition, insulin increases the proportion of biologically active testosterone by inhibiting the hepatic synthesis of sex hormone-binding globulin, the key circulating protein that binds testosterone.
In PCOS, menstrual dysfunction reflects chronic anovulation and is characterized by irregular and infrequent bleeding. There is a broad spectrum of menstrual patterns seen among women with PCOS: 5–10% may even have normal or near-normal menstrual function, whereas approximately 20% will have the complete absence of menses.
Multiple studies suggest that PCOS is heritable. For instance, a prospective study of the relatives of 195 consecutive PCOS patients found that 35% of mothers and 40% of sisters of patients with PCOS had PCOS themselves. In addition, a Dutch twin study demonstrated that concordance of PCOS was greater among monozygotic than dizygotic twins. The metabolic complications associated with PCOS are also familial. Women with PCOS have an increased likelihood of having at least one first degree relative with type 2 diabetes, and mothers of women with PCOS have increased total cholesterol and LDL cholesterol levels, as well as increased prevalence of the metabolic syndrome. The mode of inheritance for PCOS is difficult to define due to clinical heterogeneity and lack of a male phenotype, but our current understanding suggests that PCOS is a complex multigenic disorder.
Over the past decade, a large number of case–control and family-based association studies have been performed to search for candidate genes in PCOS. The most obvious genes to consider include those that may regulate the hypothalamic-pituitary-ovarian axis, as well as those responsible for insulin resistance and its sequelae. A recent review by Urbanek documented over 60 studies on the genetic contribution of more than 70 genes to the etiology of PCOS. With a few exceptions, the results of these studies have been ambiguous or lacked replication, a finding attributed to the clinical heterogeneity of PCOS and limited sample sizes.
In some instances, single gene mutations can give rise to the PCOS phenotype, as has been documented in three patients with cortisone reductase deficiency, in whom mutations of the genes for 11β-hydroxysteroid dehydrogenase type 1 and hexose-6-phosphate dehydrogenase were found. The inability to convert cortisone to cortisol, as seen with cortisone reductase deficiency, leads to the accumulation of adrenocorticotrophin-mediated androgens and mimics the phenotype of PCOS.
CYP11A Gene
One ideal functional candidate gene for PCOS is CYP11A , since it encodes the enzyme that cleaves the side chain of cholesterol p450, the rate-limiting step in androgen biosynthesis. In 1997, Gharani et al. showed evidence for linkage between the CYP11A gene and PCOS. Although additional studies demonstrated further evidence for an association between a polymorphism at the CYP11A promoter and PCOS, a subsequent large case-control study found no associations between the promoter polymorphisms in CYP11A and either polycystic ovary morphology or testosterone levels. Similarly conflicting results have been found in studies of other genes, where larger follow-up studies failed to confirm initially reported associations with the insulin VNTR gene (a regulator of transcription of the insulin) and the CAPN10 gene (involved in insulin secretion and action).
Chromosome 19p13.2 PCOS Susceptibility Locus (D19S884)
One locus that has been consistently associated with PCOS is on chromosome 19p13.2, at the dinucleotide repeat marker D19S884, which maps 800 kilobases centromeric to the insulin receptor ( INSR ) gene and is thought to be in the region of the fibrillin 3 ( FBN-3 ) gene. In addition to a structural role in connective tissue, fibrillins are also believed to regulate the activity of members of the TGFβ family. TGFh maps 800 kilobases centromeric to 19p13.2 D19S884 allele 8 (A8), within intron 55 of the FBN-3 gene. A8 was also associated with higher levels of fasting insulin homeostasis model assessment (HOMA index) for insulin resistance in women with PCOS. The association of D19S884 with markers of insulin resistance and pancreatic beta-cell dysfunction suggests that the same variant contributes to the reproductive and metabolic abnormalities of PCOS in affected women. The roles of both fibrillin 3 and its potential interactions with INSR remain an area of active research.
The Androgen Receptor Gene
In humans, the androgen receptor is encoded by the AR gene located on the X chromosome at Xq11-12. The androgen receptor ( AR ) gene and the role of X-inactivation have also received increasing attention as a possible epigenetic contributor to the PCOS phenotype. The AR gene contains a CAG repeat encoding the polyglutamine tract in the N-terminal transactivation domain. In vitro studies have demonstrated an inverse relationship between the length of the CAG repeat and receptor activity, and suggest that the length of the CAG repeat could affect androgen sensitivity. Genetic studies of the role variation in the CAG repeat, however, have not been consistent.
Since the AR gene is X-linked, other studies have found that the pattern of X-inactivation could influence AR activity and PCOS. One study looking at the pattern of X-inactivation in 88 sisters of women with PCOS found that sisters with the same AR CAG repeat genotype and the same clinical presentation (both unaffected or both with PCOS) more frequently showed the same pattern of X-inactivation than did sisters with different clinical presentations (85% vs. 16%). Thus, this study adds further support to the hypothesis that the AR CAG repeat number has an effect on PCOS phenotype.
Thus, clinical studies point to a strong heritable factor in the predisposition to PCOS, the genetic details remain poorly understood. Although the search for candidate genes will continue, the key to better understanding of complex multigenic disorders may be in expensive and large genome-wide association studies, such as those applied in type 2 diabetes.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


