Radiation oncology is a clinical discipline focused on the utilization of radiation therapy as a physical means of producing a biologic effect. The production and targeted delivery of ionizing radiation to a patient relies on the principles and accuracy of radiation physics. The goal of radiation physics is to deliver the prescribed radiation dose to a carefully identified target volume, relatively sparing adjacent normal tissues.
The biologic basis of radiation therapy includes cell- or tissue-specific inherent radiosensitivity but relies primarily on optimally exploiting differences in tumor and normal tissue responses to ionizing radiations on the basis of the time:dose relationship and modifiers of radiation response. Empiric investigations during the past century established the basis for fractionated radiation delivery protracted over several weeks to optimize differences between normal tissues and tumor in both repair of sublethal radiation injury and changes in the tumor microenvironment. The time:dose relationship is defined by the total dose (measured in Gray or Gy, the international measure of radiation, defined as that amount of radiation depositing 1 joule of energy in 1 kg, equivalent to 100 rad, the earlier term for absorbed dose where 1 rad is equal to 0.01 Gy or 1 centiGray, cGy), the number of fractions (or treatments) required to administer the total dose and the related dose per fraction, and the duration of treatment (i.e., time in days or weeks to complete the course of therapy). Technological advances in the delivery of radiation therapy and increasing experience with the interactions of radiation therapy and contemporary chemotherapy have led to more tailored utilization of radiation in children and adolescents over the past 10 to 15 years, based on the proven efficacy of local or regional irradiation and the ability to better focus radiation dose with less risk of long-term consequences. Combinations of pharmacologic agents and irradiation aim toward altering the response of the target tumor cell population or the microenvironment to enhance tumor control and/or reduce deleterious effects on normal tissues. Growing and developing tissues in children are more sensitive to late effects of irradiation than are mature, adult tissues—requiring the radiation oncologist to be cognizant of local/regional control data key to recommending radiation therapy and sophisticated in balancing the advantages of technologically advanced radiation therapy and the anticipated late morbidities that limit radiation dose and utilization.
BIOLOGICAL BASIS OF RADIATION THERAPY
Ionizing radiations interact with intracellular components within a picosecond (10-12 s) of exposure, producing both direct effects on DNA and, more commonly, indirect effects mediated by ionization of water that yields free hydroxyl radicals, which then interact with and damage DNA. Such ionization is relatively “sparsely” distributed along the path of the entrance beam for commonly used radiation beams (therefore termed “low linear energy transfer [LET],” as in photons, protons, or electrons from linear accelerators and γ rays from radionuclides used in brachytherapy—radiation implants); heavy ions deposit energy more densely and are termed high linear energy transfer radiations (e.g., carbon ions from cyclotrons or α particles in brachytherapy). DNA damage is dose-dependent and may be lethal (following accumulation of double-strand breaks, DSBs) or sublethal (e.g., for limited DSBs, single-strand breaks, cross-links, or base damage). DNA damage may be repaired via various induced cellular mechanisms including nucleotide excision repair, base excision repair, mismatch repair, and translesion synthesis; DSB break repair specifically includes homologous recombination (using a replicated chromosomal template for cells exposed following S-phase) or nonhomologous end joining (more error prone without a template for cells exposed during or before S-phase chromosomal replication).1 Repair of sublethal damage in normal cells is typically complete within 4 to 5 hours and is the basis of the therapeutic effect of fractionated irradiation. Whereas normal cells generally repair DNA damage with high fidelity, the DNA surveillance and repair pathway within tumor cells is often compromised during the process of malignant transformation. Cells progressing through mitosis with residual chromosomal aberrations (typically including dicentric and acentric chromosomal fragments) usually undergo cell death due to physical or genetic errors during cell division or result in abnormal genetic distribution in the surviving progeny that ultimately leads to cell death during subsequent divisions.2
Radiation Sensitivity
Relative cellular radiosensitivity reflects intrinsic factors, including the cell type, growth and replicative activity, cell cycle phase at the time of radiation exposure, sensitivity of apoptotic pathways, accumulation of genetic mutations in oncogenes and tumor suppressor genes, and the proficiency of DNA repair mechanisms (see previous section). Extrinsic factors determining cellular and tissue radiosensitivity reflect the complex and heterogeneous cellular composition, including stromal content, vasculature and microenvironment determining oxygenation, nutrient availability, and elimination of metabolic waste molecules.3Radiation hypersensitivity has been associated with a few genetic conditions, classically identified in children with ataxia-telangiectasia (A-T). A mutation of the ATM gene removes the usual block before radiation-damaged cells enter the cell cycle’s S phase, obviating the usual G1 arrest and DNA repair processes following DSB DNA damage, thereby greatly increasing radiosensitivity and genomic instability, the latter associated with later carcinogenesis.4 In a similar manner, in the Nijmegen breakage syndrome (NBS), cells show deficient DSB repair resulting in enhanced sensitivity to ionizing radiation.2,5,6 Multigene expression models may correlate with intrinsic radiosensitivity, providing a predictive assay of radiation response in selected tumor types.7,8,9
Classical radiation biology early recognized relationships among tumors of more primitive, rapidly dividing cells and apparent responsiveness to irradiation. The proliferating stem cell systems define much of the radiation response for tumors (where the number of clonogenic cells defines the tumor target in achieving tumor sterilization, and the number of surviving clonogenic cells may predict the likelihood of recurrence) and normal tissues (where survival of the repopulating stem cells in skin and intestinal crypts, for example, defines the degree and duration of early radiation response in these tissues).10
The Four “R’s” of Radiation Biology
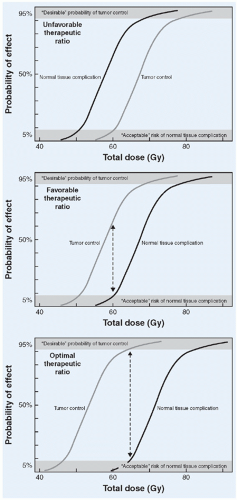
Fractionated irradiation was experimentally and then clinically found to provide tumor control while reducing the normal tissue effects associated with the single, large fractions used soon after Roentgen’s discovery of x-rays in 1895. Forty years later, cell survival assays helped elucidate the four key underlying biologic principles upon which modern radiation parameters are based: repair (primarily repair of normal tissue following sublethal radiation damage), redistribution (through the cell cycle, where cells in S-G2 phases are relatively radioresistant), reoxygenation (see below), and repopulation (where surviving tumor cells often show accelerated repopulation in response to radiation therapy, requiring a relatively brief total duration of therapy to minimize unintended repopulation during the radiation course).3 In most pediatric tumor settings, conventionally fractionated irradiation is the standard, with common total doses of 18 to 65 Gy (determined by the tumor type and presentation) delivered in five daily fractions per week of 1.5 to 2.0 Gy (most often 1.8 Gy in North America) per fraction. For pediatric cancers, a potentially controlling radiation dose can most often be administered using conventional fractionation to dose levels within acceptable tolerance limits of surrounding normal tissues, representing a favorable “therapeutic ratio” as shown in Figure 13.1.
Radiation-Induced Cell Death
Complex integrated pathways of DNA repair and cell cycle checkpoints maintain genomic integrity that is continuously challenged by spontaneous mutagenesis and genotoxic exposures. These pathways maintain cellular homeostasis by identifying cells with genetic aberrations, attempting to repair the damage, and if not repairable, setting in motion mechanisms to eliminate these cells. Cells damaged beyond repair may enter cell cycle arrest, senescence, aberrant mitosis or cell death through apoptosis, necrosis, and/or autophagy. These pathways are activated after DNA damage caused by therapeutic interventions such as radiation therapy. The precise pathway harnessed to eliminate damaged cells is dictated by the genotoxic stress and the genetic makeup of the cell.11
The tumor suppressor protein TP53 lies at the control center of these response pathways to genotoxic stress. Depending on the cell type, TP53 may induce apoptosis or stress-induced premature senescence (SIPS). Common phenotypic features of apoptosis, also known as programmed cell death, are membrane blebbing, cytoplasmic shrinkage, and chromatin condensation. The process is regulated by cysteine-dependent aspartate-directed proteases (caspases), a family of cysteine proteases that degrade key cellular proteins and culminate in cell death. The morphology of SIPS is dramatically different than that of apoptosis, with cells that remain alive and secrete growth factors but halt DNA synthesis, become large and flat, and express senescence-associated β-galactosidase (SA-β-gal).11 Radiation-induced apoptosis, mediated by TP53, presents a mechanism to exploit in enhancing radiation sensitivity.3 Accounting for cellular lethality outside reproductive cell death has been uncertain in radiation biology; several investigators have indicated that systems with a high spontaneous apoptotic rate might be more radiosensitive (requiring lower radiation doses to trigger interphase cell death).2
Oxygen State and Radiation-Induced Lethality
Intratumoral oxygenation was noted to affect radiation response early in the 1900s; later in vitro studies by Thomlinson and Gray in the 1950s showed that cells in necrotic tumor foci at the greatest distance from capillaries were viable but relatively radiation insensitive due to reduced oxygen concentration. The relative radiosensitivity of normoxic versus hypoxic cells, as defined by O2 < 3 mmHg, approximates 2.5 to 3.5 (i.e., the dose required for a given reduction in cell survival in a hypoxic environment, defined by oxygen levels is 2.5 to 3.5 times higher than when grown in normally oxygenated conditions). Molecular oxygen prevents resolution of ionizing DNA damage and can thus “fix” or make permanent free radical damage within the DNA. Moreover, the intracellular hypoxia-activated transcription factor, HIF-1, has been linked to radioresistance by upregulating cellular pro-survival proliferation pathways as well as local vascular proliferation.12 There is a marked difference in the oxygen dependency for radiation effect among low-LET radiations (photons, electrons, protons—all of which show the oxygen effect as mentioned earlier) compared with high-LET radiations (heavier particles and ions, where cell lethality is independent of oxygen content).10 During a fractionated course of radiation therapy, tumors evidence reoxygenation; this reoxygenation of chronically hypoxic, clonogenic tumor cells augments the efficacy of fractionated radiotherapy delivery. With preclinical and clinical data substantiating the impact of intralesional hypoxia on tumor control, a number of strategies have been tested to overcome hypoxia, ranging from hyperbaric oxygen to carbogen breathing (an oxygen transporter in blood) to more recent studies of vascular normalization and hypoxic cell radiosensitizers. Efficacy of such oxygen-enriching methods remains under study.13,14
Figure 13.1 Dose-response curves representing tumor control and normal tissue complication probabilities, demonstrating tumor- and tissue-specific sigmoid dose responses. Differences in dose-related effects define more or less favorable relationships. (From Gunderson LL, Tepper JE, eds. Clinical radiation oncology. New York, NY: Churchill Livingstone, 2000, with permission.)
Bystander or Abscopal Effects
There has been increasing note of radiation effects in cells outside the immediately irradiated area, the so-called bystander effects. The finding of tumor regression at sites distant to an irradiated volume was termed the “abscopal” effect. While controversial, reports of profound systemic disease response to local radiation therapy have stimulated investigation into potential mechanisms.15 Genomic instability, gene mutation, and even cell death are documented in cells not exposed to direct radiation injury, mediated by intercellular gap junctions and paracrine proinflammatory factors such as TNF-α, IL-1α, IL-1β, IL-6, and transforming growth factor (TGF-β).2,16,17 Low-dose radiation exposure (approximating 50 cGy) is associated with the release of oxygen and nitrogen radicals that can activate cells responsible for immune response (e.g., macrophages) to release cytokines.16 More extended systemic responses may be due to radiation-induced modifications in tumor cells and the microenvironment, eliciting a T-cell immune response.18 Combination of primary tumor radiotherapy with T-cell augmentation via CTLA-4 blockade has demonstrated reduction in metastatic burden in animal models.19 Several series in patients with metastatic melanoma have exploited this finding by combining local irradiation with immune-priming interventions including CTLA-4 blockade or IL-2 co-therapy with observation of abscopal responses.20,21,22
Time:Dose Fractionation in Radiation Therapy
Conventional fractionation has evolved over several decades on the basis of known tolerance and dose-limiting late effects as well as tumor control probabilities. For most centers, conventional fractionation is defined as 1.8 to 2.0 Gy per fraction, administered once daily 5 times a week to projected total doses ranging from 50 to 75 Gy. In children, the parameters are broadened at the lower range of dose per fraction, extending the lower limit of dose per fraction to 1.5 Gy for particularly sensitive tumor types, such as Hodgkin lymphoma, acute leukemias, and intracranial germinoma. Lower total doses are also used; for example, in Wilms tumor, 10.5 to 12 Gy is routine, while in acute lymphoblastic leukemia (ALL), 12 to 18 Gy may be appropriate, if radiation is used at all.
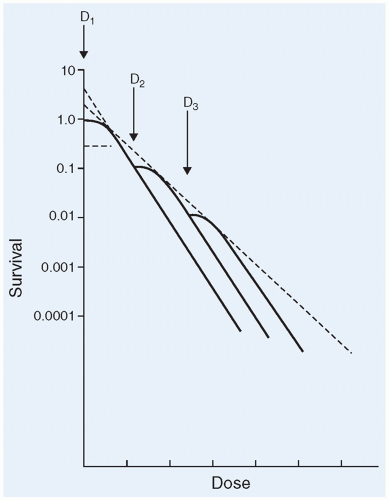
In vitro cell survival curves have long been recognized in classic radiation biology, defining a two-component linear quadratic model with an initial shoulder region (with accumulation of cell lethal effects at low doses) followed by a steeper logarithmic response at higher dose (typically >1.0 Gy) (Fig. 13.2).2 Low-dose exposures (<0.1 to 0.5 Gy) are associated with relative hypersensitivity within the shoulder region, followed by a relatively radioresistant region.23
A series of proposed isoeffect models were developed in the 1970 to 1985 time frame, demonstrating apparent equivalent biologic effects with different dose per fraction and overall treatment time relative to total dose delivered. The resultant data differ by tissue type, with steeper dose equivalent curves for dose-limiting late-responding normal tissues than for acutely responding tumor or early, self-limited acute effects. The data indicate that by reducing the dose per fraction, one can go to higher cumulative dose levels with equivalent biologic effect, and that smaller dose per fraction is likely to spare late normal tissue effects while showing little impact upon tumor control.
Figure 13.2 Cell-survival curve from fractionated radiation therapy, demonstrating repeated “less effective” dose in the initial low-dose region (“shoulder”) and the combined cell-survival effect (dotted line) reflecting less-efficient cell hill and degree of repair in fractionated deliver. (From Cohen ME, Duffner PK. Brain tumors in children: principles of diagnosis and treatment, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 1994, with permission.)
When using smaller dose per fraction, one can accommodate two fractions daily; an interfraction interval of 6 hours or more ensures virtually complete repair of sublethal damage. Relationships are tissue-dependent; for central nervous system (CNS) tissue, where the isoeffect for late reacting phenomena is quite steep compared with the impact of dose per fraction on tumor control, one can roughly equate a conventional fractionation schedule of 54 Gy delivered at 1.8 Gy once daily, 5 days per week to a hyperfractionated schedule of 66 Gy delivered at 1.1 Gy twice daily, 5 days per week. The result is equivalent normal tissue tolerance and potentially greater antitumor effect. Further dose escalation based on observed tolerance led to total doses as high as 75 to 78 Gy in Pediatric Oncology Group (POG) and Children’s Cancer Study Group (CCG) trials in diffuse intrinsic pontine gliomas between 1985 and 1995; unfortunately, the population did not include sufficient numbers of long-term survivors to confirm the lack of late effects with numerically higher total dose. Recent investigations of hyperfractionated schedules in children have sought to diminish late toxicity associated with high-dose craniospinal irradiation in advanced (high-risk) medulloblastoma; no unusual toxicities have been reported in that French SIOP trial.24 A recent study of pediatric medulloblastoma patients treated with hyperfractionation showed improved executive function, worse growth but equivalent health status, behavior, and quality of life.25
Accelerated fractionation also uses two fractions per day, but each approximates the conventional dose per fraction (1.5 to 1.8 Gy per fraction) to similar or slightly lower total doses than used in conventional fractionation—the goal here is to increase tumor control for tumors with rapid repopulation. Although rarely utilized in children, it has had some efficacy in adult head and neck cancers.26
There are data indicating the importance of overall treatment duration (time) (or avoiding interruption of a conventionally fractionated schedule), most apparent in pediatrics in medulloblastoma, where prolonged duration of therapy (i.e., interruptions adding days to complete irradiation) negatively impacts disease control.27 For some of the uniquely sensitive tumors (e.g., Hodgkin lymphoma, germinoma), the duration of therapy does not seem to impact disease control.
PHYSICAL BASIS OF RADIATION THERAPY
Ionizing radiation interacts directly with intracellular macromolecules or, more often, indirectly by electron or intranuclear ionization that results in energetic charged particles capable of breaking physical and chemical bonds. The greatest advances in radiation therapy provide sophisticated means of conforming a high-dose radiation volume to the defined tumor target and increasingly sparing critical normal tissues. The convergence of three-dimensional (3-D) imaging identifying the targeted region in anatomic space, 3-D planning for radiation delivery, automated beam direction and shaping, and confirmatory “online” imaging allows optimization of radiation planning and delivery in a way that best provides target coverage while limiting “unintended dose” to critical normal tissues. The advances in radiation delivery alone over the past 10 to 20 years have spurred much of the enthusiasm to better utilize radiation therapy in children rather than avoiding a modality that offers considerable efficacy, with increasingly better defined and less pronounced morbidities.
While radiation therapy plays a key role in the treatment of pediatric tumors, delivery of adequate therapy must always be balanced against potential treatment-related toxicity. As radiation therapy has evolved, treatment modalities have emerged that allow for more precise planning and delivery. Advances in imaging technologies, including magnetic resonance imaging (MRI) and computed tomography (CT), have allowed better identification of both tumor and surrounding critical structures. The development of three-dimensional conformal radiation therapy (3DCRT), and more recently, intensity-modulated radiation therapy (IMRT), have allowed clinicians to decrease doses delivered to critical structures while maintaining or increasing doses delivered to the tumor. While the concept of conformal therapy is not new, dramatic improvements in the power and availability of computers have allowed more complex treatment planning systems. The advent of other technical advances such as multileaf collimation (MLC), digitally reconstructed radiographs (DRRs), and electronic portal imaging have contributed to the integration of conformal radiation delivery. These advanced techniques are considered standard in most first-world radiation therapy centers and require multiple well-coordinated steps.
External Beam Irradiation
Therapeutic radiation can be delivered using external beam irradiation, such as photons, electrons, and charged particles produced by a machine outside of the body, or using internal radiation or brachytherapy from radioactive material placed in the body.
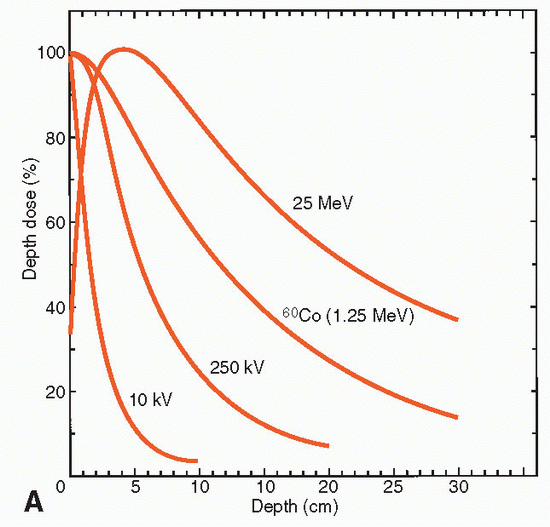
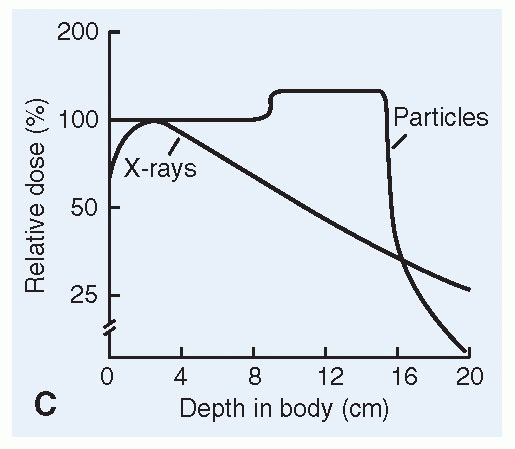
Photon therapy is electromagnetic radiation such as high energy x-rays that causes tissue interactions and DNA damage in the targeted atoms. X-rays can be considered as packets of energy that are produced at relatively low energy for diagnostic x-rays (typically 50 to 140 kilovolts [kV]) and at high energy for radiation therapy (˜ 6,000 to 25,000 kV or 6 to 25 megavolts [MV]). Photons are produced by linear accelerators by injecting electrons into a wave guide that continuously accelerates the electrons by reversing charged plates to ultimately produce an electron beam of up to 6 to 25 mega electron volts (MeV). The electrons then strike a target that stops the beam instantaneously, resulting in Bremsstrahlung or x-rays that are then channeled to exit through flattening filters and collimators that define a medical photon beam. Photon energy is absorbed exponentially in tissue; the rate of absorption in tissue and the degree of penetration are determined by the beam energy (Table 13.1). The energy of an incident photon beam of 6 MV, for example, is absorbed to 50% of the entry dose by 14 cm; for a 15-MV beam, the dose at 14 cm is 70% of the incident beam. Techniques using MLCs and IMRT allow for the exact configuration of specific beam trajectories to together encompass the desired tumor target in three dimensions and reduce collateral damage of neighboring tissues.
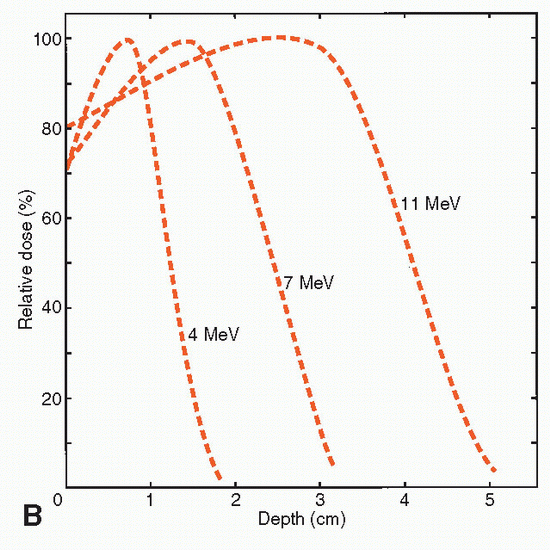
Electron therapy is a type of radiation that is absorbed more superficially, essentially penetrating to a given, limited depth based on the beam energy. The distal falloff in tissue is relatively narrow, hence avoiding certain tissue damage beyond its penetration. For example, a 6-MeV electron beam has a relatively flat dose deposition of dose between 100% dose measured just beneath the entry surface and 90% of dose delivered at 2 cm into the tissue, at 4 cm. The dose drops to only 10% of the maximum dose at 4 cm into tissue. For a 15-MeV electron beam, there is relatively flat deposition of dose to 4 cm of tissue, and only 10% remains at 7 cm depth (Table 13.1). Electrons are also produced by linear accelerators, essentially extracting the electron beam directly by removing the target used to create the Bremsstrahlung effect.
Protons are high-energy, charged particles of particular interest for pediatric cancer treatment, given the potential for decreased normal tissue damage. As compared with photon beams, interest in proton beam radiation therapy (PBRT) reflects the relatively favorable physical dose distribution, which includes the potential for somewhat decreased entrance dose, and importantly, a significantly reduced exit dose because of the proton beam’s sharp distal falloff beyond the target region. Protons can enter at 20% to 30% of the maximal dose and reach maximal dose only as they slow at a predetermined depth in tissue as defined by the beam energy. As the proton beam energy increases, the depth of penetration increases. As the protons reach their suggest of maximum tissue penetrance, they deposit 100% dose as a Bragg peak at which suggest, nearly all of the energy is absorbed in matter. Following this peak, there is almost no further penetration and no exponential exit dose unlike photon beams (Table 13.1).
Proton beams are produced by high-energy cyclotrons. The width of the beam is determined by the largest dimensions of the target volume perpendicular to the direction of the proton beam. A single depth of a target volume is treated by a specified incident proton energy producing a Bragg peak at a particular depth. By modulating the energy of the proton beam, multiple Bragg peaks at different depths are combined to form a “spread out” Bragg peak (SOBP) covering the full range of depth in the target. In the modulated beam, the entrance dose (superficial to the target) is approximately 70% to 80% of the maximal Bragg peak dose (Table 13.1). [See the following section on Radiation Treatment Planning (RTP)].
Most currently available PBRT centers use passive scatter or uniform scan beam technology, essentially producing a single proton beam of given energy that requires beam compensators (to correct for tissue inhomogeneities within the planned path of the beam) and physical “blocks” to shape the beam to the contour of the target from that trajectory. Both devices generate neutron contamination, although far more neutron contamination is generated in passive scatter as opposed to uniform scanning beams. The neutron contamination is a concern regarding secondary carcinogenesis as summarized later. Pencil beam scanning beam technology is now used at various centers, including the Paul Scherrer Institute in Switzerland; the beam is electronically shaped and modulated to allow for an even more conformal dose distribution without significant neutron contamination.
TABLE 13.1 Characteristics of Medically Useful Radiations
Skin-sparing; slow falloff in dose with depth; absorption independent of tissue density (60Co, 4-10 MeV x-rays); linear accelerator offers superior beam definition
Uniform RBE of 1.0 throughout depth; effectiveness oxygen-dependent
Most common modality for local and wide-field irradiation
Electrons
Linear accelerator (>10 MeV)
Plateau of dose superficially within tissue (1-5 cm); effective range in tissue energy-dependent; increased absorption in bone; relatively poor beam definition
Identical to photons
Often combined with photons for superficial tumors (e.g., parotid bed rhabdomyosarcoma) or to limit dose to a superficial structure (e.g., eye retinoblastoma)
Protons
High-energy cyclotron or synchrotron (>160-250 MeV)
Plateau dose distribution with modulated physical (Bragg) peak; depth of peak and range in tissue distinct and energy-dependent; absorption independent of tissue density; excellent beam definition
RBE of 1.1; relative oxygen independence
Favorable dose distribution with modulated energies (to broaden the Bragg peak); idealized volume coverage for pediatric CNS tumors (local and potentially for craniospinal irradiation), pediatric sarcomas
Heavy charged particles (“stripped nuclei” of carbon, neon, argon)
High-energy cyclotron or synchrotron (>500 MeV)
Similar to protons
RBE of 1.5-3; Bragg peak RBE for hypoxic cells of 2.5-5; oxygen independence similar to neutrons; late similar to neutrons; late effects in children (CNS, somatic) not yet determined
Focal tumors (e.g., ocular lesions); deep-seated tumors with hypoxic foci and/or potential dosimetric gain re photon therapy (e.g., retroperitoneal, pediatric CNS tumors)
Neutrons
Cyclotron (>7-14 MeV)
Similar to 60Co teletherapy; relatively unfavorable depth-dose characteristics and beam definition
Similar to photons (60Co)
RBE of 2-8, varies with dose per fraction; dependence on oxygen is one-third to one-half that of photons
Mixed with photons for tumors with known necrotic (hypoxic) fractions (most effective in salivary gland tumors or soft tissue sarcomas in adults; limited enthusiasm for use in children 2° apparent increase in carcinogenicity in the young
RBE, relative biological effectiveness (RBE = 1 for 250 kV orthovoltage x-rays); CNS, central nervous system.
a Beam definition refers to sharpness of field margins in tissue.
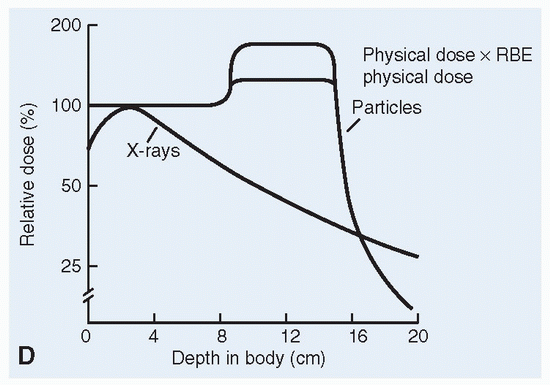
In terms of biologic dose delivered, protons are essentially equal to photons biologically and are also considered a low LET beam. Measured radiation effect in vitro is used to compare biologic effectiveness of different physical beams, the comparative metric called the relative biologic effectiveness (RBE). With megavoltage photons as 1.0, the RBE of protons is estimated at 1.1; proton dose is often measured in “Cobalt Gray Equivalents” (CGE) to allow for easier comparison to photon (cobalt) dose. For example, 1 CGE of protons is 0.91 Gy of protons.28 There are some uncertainties related to the proton RBE at the distal edge of the SOBP, with concern of increased effects on normal tissues at that depth.
Heavy charged ion therapy includes carbon, neon, or other elements in which the electrons have been stripped away during cyclotron acceleration. The mass of the ions exceeds that of protons. Such heavy particles potentially have a narrower Bragg peak and the RBE is higher with greater LET in the target region. Hence there is interest in heavy ions as they can theoretically provide greater tumor effects without significantly increased normal tissue damage (Table 13.1). Since the LET is high in the targeted Bragg peak region, there is little oxygen dependency for heavy charged ions.29 There are currently few centers planning heavy charged ion irradiation, but the potential for yet more conformal physical and biological delivery warrants future interest. Some consider carbon potentially the best option since it maintains a narrow Bragg peak, low fragmentation tail, and high RBE effect.30 There is a radiobiologic concern that the use of carbon in pediatric cases may increase the risk of treatment-induced secondary cancer.31 Hence, to date, the use of carbon in pediatrics has been limited, including use in radioresistant tumors, for critical or inoperable locations such as skull base tumors, and in combination with protons, or in lieu of protons if the greater RBE effect was desired or if protons were unavailable.30
Neutrons are heavy particles without charge. Although offering no physical advantage in dose distribution over photon irradiation, “fast neutrons” (7 to 14 MV) are of interest because neutron interactions in tissue are not oxygen dependent. Neutrons have an estimated RBE of 2 to 8 compared with photons or protons, with some variation in the RBE based on dose per fraction and the tissue or tumor affected. Neutron trials just after World War II resulted in unacceptable morbidities, as the variation in RBE was not appreciated. Subsequent trials suggest a benefit when neutrons are used for adult salivary gland tumors. Neutrons are not recommended for children, on the basis of atomic bomb data suggesting that children are particularly sensitive to added carcinogenic risk from neutron irradiation. Neutron capture therapy has long had some interest for adult neurosurgeons. Low-energy neutrons (0.1 eV to 10 KeV) are absorbed by intratumoral boron to result in unstable radionuclides that immediately undergo disintegration, bathing the local tumor region with energetic, high-LET radiations. This has not had a significant role in pediatric treatment.32,33
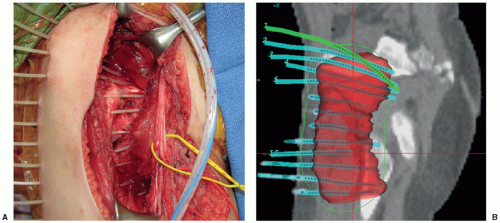
Figure 13.3 A: Intraoperative photograph showing operative bed following resection of a high-grade synovial sarcoma of the thigh. Note indwelling catheters inserted in the perpendicular plane to provide coverage for microscopic residual with planned postoperative brachytherapy. Catheters are left in place with accessible end that can be easily attached to high-dose rate unit. B: Dosimetry displaying operative bed (red detail in three dimension), reference isodose volume (green line just beyond red volume) that indicates the region of tumor bed and adjacent microscopic margin covered by intended dose, and catheters (with 192Ir seeds indicated as dark lines within the catheters). The reference isodose volume here received 34 Gy given in 10 fractions of 340 cGy twice daily; each application took 11 minutes. (Courtesy of M. Krasin.)
Brachytherapy
The use of radioactive implants or molds provides direct applications of local radiation therapy (or brachytherapy) through interstitial (within tissue), intracavitary (within body cavities, in pediatrics, primarily vaginal or nasopharyngeal), or surface mold (ocular plaques or molds conformed to operative beds) techniques. Radioactive sources are placed directly within or adjacent to the tumor or tumor bed, essentially resulting in “internal” irradiation that delivers a high radiation dose precisely within a confined planning volume with rapid falloff in dose over a very limited distance beyond the application. The dose distribution in brachytherapy applications is governed almost entirely by the inverse square law, explaining the rapid falloff in effective dose (Fig. 13.3). Implants are also completed over a relatively short time frame, typically within 3 to 5 days.
In practice, brachytherapy is limited to tumor beds less than 5 to 10 cm in maximal dimension. The most common uses in pediatrics are for soft tissue sarcomas: rhabdomyosarcomas in specific locations (extremities, vagina, less often head and neck region) and, more commonly, the other soft tissue sarcomas occurring in extremities or along the trunk (synovial cell sarcomas, fibrosarcomas, epithelial cell sarcomas, etc.).34,35,36 Afterloading catheters are placed into the tumor bed during surgery for interstitial implants. After a 3- to 5-day immediate postoperative interval to allow healing, radioactive sources are positioned within the catheters at predefined locations to deliver the planned dose within the targeted volume of the implant. Classically, most applications in pediatrics have been manually placed, removable low-dose rate exposures using radioisotopes to deliver γ rays (equivalent to photons) at 40 to 90 cGy per hour to a total of 20 to 50 Gy over a continuous exposure time of 2 to 5 days. Such low-dose rate brachytherapy utilizes iridium 192 (192Ir) or iodine 125 (125I), emitting γ rays of 380 keV or 30 keV, respectively. 192Ir provides somewhat more homogeneous dose distributions, especially within larger implant volumes, if exposing more peripheral tissues (outside the target volume) to low radiation doses. 125I has the advantage of more limited penetration and is particularly useful in ocular implants and in young children.
When used as primary postoperative irradiation, a total dose approximating 45 Gy has been typical for most soft tissue sarcomas; when used as a local “boost” within a larger volume treated by external beam radiation therapy (to more broadly cover areas of potential microscopic extension for larger or more infiltrating tumors), an implant dose of 20 to 30 Gy is usually planned.35 Surface applications, most often as radioactive plaques in focal ocular irradiation for retinoblastoma, use strategically located radioactive seeds imbedded within a gold plaque that is placed directly under the targeted retinal site during surgery and left in place for 3 to 5 days depending upon the planned dose and the dose rate.
For interstitial and intracavitary applications, most centers now utilize high-dose rate remote afterloading applications that are repeated on a daily or twice-daily schedule.37 Remote afterloading equipment provides a self-shielded array of 192Ir sources that are programmed to deliver sources of predetermined length to respective indwelling catheters for time intervals determined by detailed patient-specific, CT-based dosimetry. Each application lasts only several minutes; since the catheters or mold are already in position and relatively little manipulation is required to secure the catheter connections to the remote afterloading device, the applications require sedation only for very young children. Experience in pediatrics has typically used 340 cGy delivered twice daily for a total of 3.4 Gy (3,400 cGy) in 10 applications over 5 to 7 days when treating with brachytherapy alone (biologically equivalent to 45 Gy administered via low-dose rate implant) or 300 cGy delivered twice daily for a total of 21 Gy (2100 cGy) in seven applications over 4 to 6 days when used as a boost (biologically equivalent to 30 Gy low-dose rate brachytherapy).35 Single applications of highdose rate brachytherapy have been utilized to provide “boost” irradiation to the tumor bed at the time of surgery, particularly in retroperitoneal, pelvic, or deep-seated extremity sarcomas—a form of intraoperative radiation therapy. Such applications allow precise localization and, often, the ability to physically relocate adjacent bowel or kidney away from the radiation implant, further protecting adjacent critical structures.
Radioactive colloids can be instilled directly into cyst cavities, primarily in primary or “salvage” therapy for craniopharyngiomas or, less often, cystic astrocytomas. 32P, 90Y, or 186Re are pure β emitters with extremely limited penetration in tissue (0.5 to 1.5 mm) providing high doses to the internal cyst wall (200 Gy at the surface). The procedure requires technical experience, wherein the targeted cyst(s) is reduced by aspiration, the volume then calculated based on CT or MRI, and physical algorithms employed to determine the amount of colloidal radionuclide that is instilled via stereotactically placed catheter to provide the prescribed dose. Given the short range of β radiations, the key vital structure potentially in range is the visual apparatus (optic nerves, chiasm). In centers adept at this type of intervention, this approach has been safe and effective, with rare reports of late visual loss.38,39 In addition to minimizing dose to critical structures such as the chiasm, less dose is delivered to the developing brain which may minimize neurocognitive deficits and potential for secondary malignancies. This technique may also be beneficial in patients who have received prior irradiation in which maximum doses to critical structures has already occurred.
Stereotactic Radiosurgery
There are several stereotactic techniques that deliver a precise, relatively small volume of irradiation based on stereotactic coordinates (3-D, image-guided targeting to a defined suggest in space), precise localization and immobilization, and CT and/or MRI with stereotactic frame or fiducial markers in place. Classical radiosurgery is analogous to a surgical procedure, delivering a single high dose of photon irradiation that causes cell death and necrosis within the targeted volume. The procedure relies on the immediate cytolethal effect. With no fractionation, there is no biologic sparing of normal tissues within the targeted volume.40,41 Initial applications of radiosurgery were limited to intracranial targets, using the Leksell Gamma Knife ®, a stand-alone radiosurgical device based on triangulating the spherical target defined by collimation and stereotactic positioning to produce a spherical target from 200 60Co sources strategically placed within a shielded structure. This technique is still widely used to treat a variety of intracranial tumors or benign processes such as arterial venous malformations (AVM). During this procedure, a frame is placed prior to treatment and imaging and is used both as a reference suggest allowing precise radiation delivery based on imaging obtained for planning and to lock the patient position during treatment. The frame allows minimal movement and therefore, margin is often not necessary during single fraction treatments. Treatment time is dependent on the complexity of the plan and can range from 15 minutes to several hours. Often, anesthesia is needed and is done prior to frame placement and imaging.
Modified linear accelerators can also deliver radiosurgery.41,42 Frameless technology, including CyberKnife®, is based on coordinated orthogonal imaging and both a treatment couch and small, “portable” linear accelerator free to move through all trajectories and locations in 3-D space with fixed anatomic points or surgically placed fiducials to allow real-time image-guided exposure. Both frameless linear accelerator approaches and CyberKnife® permit single- or multiple-fraction radiosurgery, the latter often termed stereotactic radiotherapy.43
Most pediatric experience has been in recurrent tumors, particularly ependymomas and glial neoplasms; as a part of primary therapy, radiosurgical “boost” has been added when standard radiation management and chemotherapy have not achieved early “complete response,” particularly in ependymoma, malignant germ cell histiotypes, and high-grade gliomas.40,44,45 A few dedicated radiosurgical centers have explored broader use as primary radiation management where anatomic geometry allows high-dose radiosurgery while avoiding excess exposure to critical normal structures. Notably, experience with craniopharyngiomas has been of interest, if not broadly adopted.46 In children with low-grade CNS tumors as a part of neurofibromatosis (NF) (typically type 1 with optic pathway gliomas or tumors located in nonsurgical sites such as the midbrain; also, type 2 with acoustic neuromas), judicious use of radiosurgery has often provided early disease control while preserving broader CNS “radiation tolerance” in anticipation of later requirements for radiation therapy.40,41,47
Radiosurgery has been used for benign conditions as well such as pediatric arteriovenous malformations (AVM).48 Potts et al. presented a single institution experience using gamma knife for pediatric AVMs with a median dose of 17.5 Gy and found that AVM obliteration was achieved in 52% of patients who received a dose of 18 to 20 Gy (16% who received less than 18 Gy). They reported no permanent neurological deficits in patients who did not experience posttreatment hemorrhage.
With the availability and documentation of precise patient localization and dose deposition, current interest has focused increasingly on spinal body or paravertebral irradiation using rapid fractionation (single exposures or limited number of fractionated treatments) based on what is termed “body radiosurgery.”49 Applications in children have focused primarily on vertebral body irradiation for metastatic disease.
Technical Basis of Radiation Therapy
The ability to better focus radiation dose reflects the introduction of more sophisticated technologies. Cross-sectional imaging (CT, MRI) can be imported into RTP systems, enabling 3-D reconstructions or using 3-D MR acquisitions to define overt tumor volumes. The ability to incorporate more detailed anatomic information is integral to accurate radiation planning. Key in this first step of RTP is registering MRI and/or positron emission tomography (PET)/CT imaging to the CT data set that provides the basis for dose calculation. The CT data are obtained at simulation—the start of RTP when the patient is positioned ideally for treatment delivery. During this step, appropriate molds or casts are formed that both allow the patient to be comfortably positioned for therapy and ensure daily reproducibility of the setup and maximal immobilization during treatment. Critical anatomic regions (target volume and/or critical structures) are based on the most informative imaging modality.
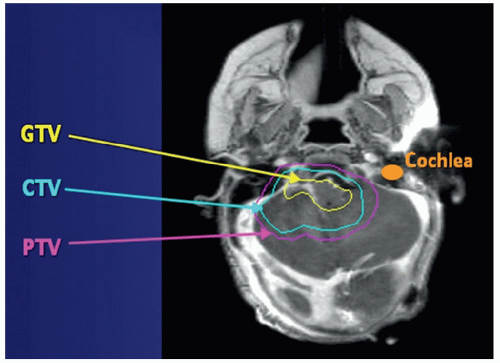
Diagnostic or radiation therapy-specific MRI or PET/CT studies can be fused to the simulation-obtained reference CT scans. Stereotactic localization based on fiducial markers inserted at the time of surgery or during simulation provides reference points used during simulation and are available for “real-time” confirmation or adjustment of patient position during daily irradiation. RTP continues as the physician outlines the gross tumor volume or GTV, typically the initial tumor extent or the postoperative tumor bed as tissues may have reconfigured after surgery. Less often, postoperative or post-chemotherapy volumes are used to define the GTV, using the residual tumor after chemotherapy or the operative bed and overt residual after surgery. The area(s) of potential microscopic extension (by direct infiltration and/or regional draining lymph nodes) define the expansion of the GTV to form the clinical target volume or CTV. In most settings, the CTV is determined by a given 3-D expansion of the GTV (e.g., 0.5 to 1 cm or more), corrected for anatomic interfaces to identify the final CTV (Fig. 13.4). In practice, the CTV is defined by our best understanding of the degree of tumor infiltration likely in a given direction and then limited by adjacent skull or the midline (falx) or compartmental barrier (e.g., the posterior fossa-defining tentorium in the brain; the mediastinal-pleural surface in targeting thoracic lymph nodes, barriers through which tumor is unlikely to extend). One might expect considerable infiltration of osseous Ewing sarcoma within the involved medullary cavity, requiring a greater expansion to define the CTV than in a clear cell sarcoma of the kidney, where margins for microscopic extension beyond the renal capsule might be only 1 cm. The CTV can also include the immediately adjacent or regional lymph nodes in tumors known to spread via the lymphatic system. Once the CTV is established, a simple geometric expansion of the CTV by 3 to 10 mm provides the planning target volume or PTV. The PTV accounts for variation in daily patient setup or any potential movement during therapy (organ movement or degree of patient immobilization). Daily imaging on the treatment table (image-guided radiation therapy) in which patient position is adjusted by millimeters can reduce the setup uncertainty, with accompanying decreased size of planning target volumes (Fig. 13.4). Dose within the tumor target can be quite homogeneous or show intralesional variations in dose, based on MR spectroscopy or PET to identify regions of greater proliferation or metabolism or focal areas of hypoxia, regions that may require higher radiation doses than otherwise “less active” or “euoxic” areas within the tumor.50,51
Figure 13.4 Defining target volumes for pediatric radiation therapy: the gross tumor volume (GTV) here defines the operative bed and residual tumor for a IVth ventricular ependymoma that surrounded the brainstem and involved the right foramen of Lushka, on the basis of preoperative MRI and postoperative shift in brain tumor structures; the CTV is a 1-cm 3-D anatomic expansion of the GTV, here corrected for anatomic barriers (the anterior aspect of the tentorium and the prepontine cistern); the PTV is a strict geometric 3-D expansion of the CTV, here using 3 mm for a child treated in an immobilizing mask and sedated (to virtually eliminate movement during therapy). (Courtesy T. Merchant.)
In addition to target volumes, treatment planning requires identification of critical normal tissues. In developing a treatment plan, one identifies a dose or range of doses sought in the PTV, sometimes recognizing two or more PTVs with different intended dose or doses (e.g., for embryonal brain tumors, a dose of 23.4 or 36 Gy is often prescribed for the entire neuraxis, while the “primary tumor bed” dose is 54 Gy; for nasopharyngeal embryonal rhabdomyosarcoma, a dose of 36 to 41.4 Gy is typically sought for the nodal region of initial involvement that responded completely to chemotherapy, while the primary tumor dose is 50 to 55 Gy). Limits are defined for critical structures: in the two prior examples, one would plan to limit the dose to the chiasm to 50 Gy (in both supratentorial embryonal CNS tumors and in nasopharyngeal rhabdomyosarcoma) and the spinal cord to 40 to 45 Gy (in nasopharyngeal tumors where the primary tumor and residual nodal disease require 45 to 55 Gy and are often contiguous with the spinal cord).
Three-Dimensional Treatment Planning and Delivery: Three-Dimensional Conformal, Intensity-Modulated Radiation Therapy
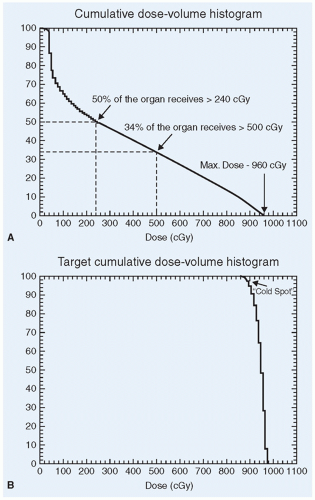
Standard pediatric radiation therapy requires 3-D conformal planning/delivery (3D-CRT), anticipating that in certain presentations IMRT may offer advantages.50,52 Following target volume definition, RTP proceeds to dosimetry: determining the array of radiation beams that each provides a proportion of the dose, including the specific trajectory through which a beam enters the body, encompasses the target (based on the “beam’s eye view” of the target’s shape and size through the angle at which the beam encompasses the target), and exits beyond the target volume. Sophisticated calculation and display systems enable one to plan and optimize plans that conform the radiation dose to the target along with estimates of the intervening and post-target exiting dose contributed by each field. As RTP has advanced to more complex field arrays and weighting, the display of target and organ dose uses a format known as dose-volume histograms, graphically depicting the radiation dose received by subtended volumes of the identified structure (tumor target or normal tissue) (Fig. 13.5).
In 3-D CRT, a number of trajectories are identified that encompass the PTV and minimize or avoid traversing identified critical normal tissue structures. Each of the beams is shaped to include the size and shape of the target volume in the plane with which the beam intersects the PTV (the so-called beam’s eye view). One or more of the beams may include a manual or electronic wedge that modifies the dose across the beam when such will improve the composite dose distribution that accounts for all beams and the body contours through which they traverse. 3-D CRT typically results in highly uniform dose distribution throughout the PTV.
Figure 13.5 Dose-volume histograms (DVH). A: Nominal DVH indicating dose received in given percentage of indicated structures. The amount of information available in describing three-dimensional dosimetry requires a graphic display to appreciate the relative dose in varying portions of an identified target or normal structure. B: For tumor, DVH indicates more than 90% of the projected dose within the identified target; the “cold spot” identifies less than 10% of the target’s volume receiving less than 90% of the targeted dose.
The basis of IMRT is to further optimize radiation therapy to improve the tumor control probability by increasing dose to the target volume while diminishing the likelihood of normal tissue complications by allowing specified dose limits to critical normal structures. While 3D-CRT allows the high-dose region to conform to the target volume to a much greater extent than does the traditional 2-D or planar planning, it is limited in situations where anatomy creates a concave interface between target and normal structure (e.g., around the spine) or where specific structures adjacent to the target volume require relative underdosing (e.g., the cochlea when treating the posterior fossa or a tumor bed within that region, or the spinal cord adjacent to a soft tissue sarcoma). In such circumstances, IMRT offers the advantage of “sculpting” the dose around a given “avoidance” structure.53 Through multiple beam trajectories, each including multiply shaped, differently weighted “beamlets” that provide “modulation” of dose within the 2-D beam view of each beam angle, one can create a 3-D dose plot that obeys the constraints of minimal and maximal dose within a target volume that has closely conformed dose with (a) greater internal inhomogeneity (specifically, regions of greater dose intensity than one sees with 3D-CRT) but (b) specific areas of “underdosage” as prescribed in adjacent normal tissue structures. 3,38 IMRT delivery requires an MLC aimed through a large number of gantry angles with beam modifications at each trajectory. The result is increased treatment time and complexity, requiring greater attention to immobilization (for children, often sedation/anesthesia) to ensure accurate delivery. Dose delivery through optimized IMRT is quite precise and, when administered in a program that includes image-guided radiation therapy (IGRT, see later), can achieve idealized dose conformality to the intended target and meet the demands of limiting normal tissue doses to prescribed dose levels. The longer “beam on” interval and inherent if “minimal” leakage through the MLC result in greater incidental dose to remote normal tissues—resulting in larger normal tissue volumes exposed to very low radiation doses.54 Specific studies in children show somewhat less unintended dose from IMRT techniques as field volumes are often smaller than in adults. This is important as survivors of childhood cancer are at risk for late secondary carcinogenesis often related to low-dose radiation exposures.55,56,57
Proton Beam Radiation Therapy
IMRT provides excellent dose distribution for most pediatric settings based on widely available linear accelerators. PBRT can often further spare normal tissues, a significant advantage in children with CNS tumors and several other presentations. The physical characteristics of the charged proton beam are discussed earlier; key is the lack of exit dose, sparing underlying normal structures any radiation exposure.27,54,58,59
Recently, the body of literature regarding proton therapy for pediatric cancer patients has been growing, composed mostly of dosimetric studies and case series. Much of the benefits ascribed to proton therapy are associated with treating CNS tumors, although potential benefits in treating non-CNS tumors are also reported. Dosimetric studies of craniospinal irradiation show reduction of dose to cardiac structures that may decrease late cardiac risks,60 to breast tissue likely lowering risks of secondary breast tumors,61 and to ovaries allowing for preservation of hormonal and reproductive function.62,63 Similar comparisons from St. Jude show moderate reductions potentially contributing to mitigation of intellectual deficits: in treating localized optic chiasmatic/hypothalamic astrocytomas or craniopharyngiomas, PBRT significantly reduces the volume of normal brain exposed to low- and intermediate-dose levels in the temporal lobes, dose levels associated with IQ effects in related radiation models.59,64 Even with posterior fossa ependymomas, where the CTV and PTV expansions require a margin of only 1 to 1.5 cm, substantial sparing of the temporal lobes is seen with PBRT.59 In craniospinal irradiation, exit exposures from posterior spinal fields can be meaningfully reduced: dose received by 50% of the cardiac volume is reduced from 72% of the PTV dose to 0.5% comparing standard photon irradiation to PBRT.58 Similar or greater reductions have been reported in paraspinal sarcomas in adults, relevant to common pediatric presentations (e.g., neuroblastoma, vertebral Ewing sarcoma).65 In retinoblastoma, more than 5 Gy is delivered to 25% to 70% of the bony orbit with a variety of 2-D and IMRT photon plans compared with 10% with PBRT.66 In pediatric pelvic sarcomas, the dose to the ovaries and pelvic bones can be substantially reduced depending on the anatomic location and size of the tumor.66
Only gold members can continue reading. Log In or Register to continue