further because these patients have a history of nasal polyps, which produce similar symptoms. Tumors of the maxillary antrum also tend to remain silent until they extend outside the sinus. As a result of tumor extension to the premaxillary region, patients can complain of facial pain, numbness, localized swelling, nasal obstruction, and epistaxis. Nasal obstruction from tumor extension to the nasal cavity and tumor extension into the orbit causing ocular problems such as epiphora, proptosis, diplopia, eye pain, and inner canthal mass are the most common symptoms of ethmoid sinus tumors. Sixth nerve palsy, severe morning headaches, and diplopia are common symptoms for primary sphenoidal tumors. Lastly, frontal sinus tumors can present with bilateral swelling of the glabella and the supraorbital ridge and with frontal pain.
TABLE 21.1 Seventh Edition of AJCC Staging for Nasal Cavity and Paranasal Sinus Cancer | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
the olfactory nerve, which innervates the superior nasal concha and upper third of the septum.
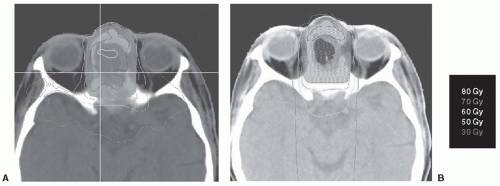 FIGURE 21-1. An example of an ethmoid sinus tumor being planned using (A) IMRT and (B) 3D-CRT. Notice that the 70-Gy isodose line (dark blue) coverage is superior in the IMRT versus the 3D-CRT plan. In addition, there is superior sparing of the optic chiasm when compared with the 3D-CRT plan. IMRT, intensity modulated radiation therapy; 3D-CRT, three-dimensional conformal radiotherapy. (See color insert.) |
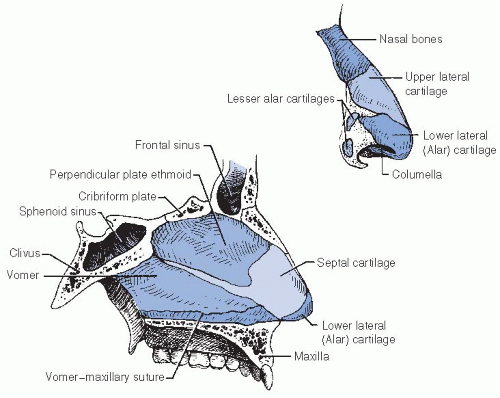 FIGURE 21-2. Relationship of bones and cartilages of the nose. Source: From Milton RR, Cassisi NJ, Wittes RE. Cancer in the head and neck. In: Devita VT Jr, Hellman S, Rosenberg SA, eds. Cancer: Principles and Practice of Oncology. 2nd ed. Philadelphia, PA: JB Lippincott Co; 1985: 407-506, with permission. |
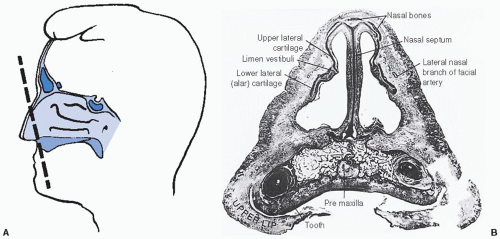 FIGURE 21-3. A: Coronal whole-organ section through the vestibule. B: The upper lateral alar cartilages fuse with the cartilaginous septum. The nasal bones overlap the upper and lower cartilages. The limen vestibule is the junction of the upper and lower lateral cartilage. Source: From Bridger MWM, van Nostrand AWP. The nose and paranasal sinuses—applied surgical anatomy: a histologic study of whole organ sections in three planes. J Otolaryngol. 1978;7(suppl 6):1-30, with permission. |
TABLE 21.2 Kadish Staging of Esthesioneuroblastoma | ||||||
|---|---|---|---|---|---|---|
|
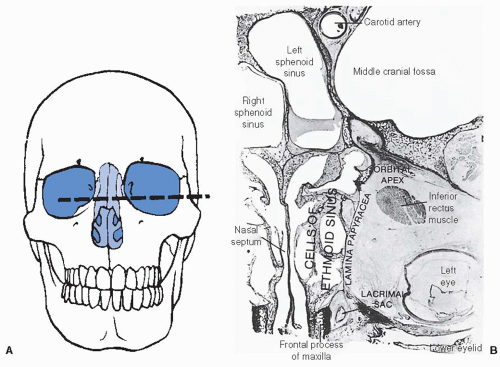 FIGURE 21-4. A: Horizontal section through the lacrimal sac, the orbit, and the ethmoid and the sphenoid sinuses. B: The posterior ethmoid cells extend farther laterally than the anterior cells. The sphenoid sinus is in close relationship to the optic nerve and the orbital apex. Note the short distance between the anterior ethmoid sinuses and the inner canthus. Source: From Bridger MWM, van Nostrand AWP. The nose and paranasal sinuses—applied surgical anatomy: a histologic study of whole organ sections in three planes. J Otolaryngol. 1978;7(suppl 6):1—30, with permission. |
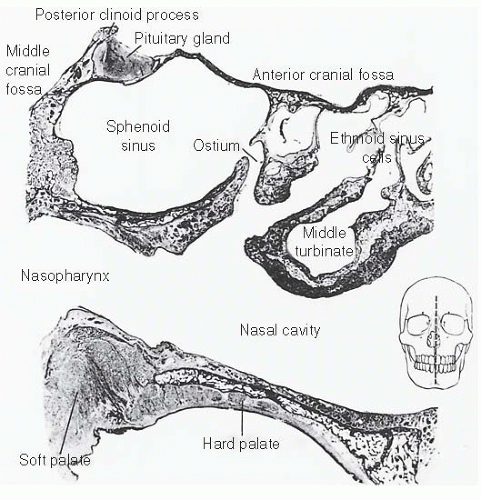 FIGURE 21-5. Sagittal section through the nasopharynx and the sphenoid sinus, just left of midline. Note relationship of the sphenoid sinus ostium to the nasopharynx and the posterior nasal cavity. The anterior wall of the sphenoid sinus and the floor of the sella are thin bone. Source: From Bridger MWM, van Nostrand AWP. The nose and paranasal sinuses—applied surgical anatomy: a histologic study of whole organ sections in three planes. J Otolaryngol. 1978;7(suppl 6):1—30, with permission. |
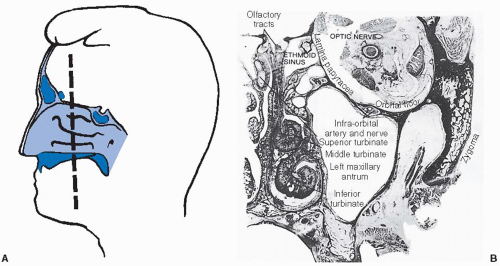 FIGURE 21-6. A: Coronal section through the maxillary antrum. B: Note the thinness of all walls except the hard palate. Lateral to the antrum is the buccinators muscle and fat pad. Source: Modified from Bridger MWM, van Nostrand AWP. The nose and paranasal sinuses—applied surgical anatomy: a histologic study of whole organ sections in three planes. J Otolaryngol. 1978;7(suppl 6):1-30, with permission. |
of proper sites to be irradiated must be considered. For example, for patients with tumors at risk for perineural spread such as adenoid cystic carcinomas, the planned target volume should include the neural pathways up to the cranial nerve ganglion at the base of skull.
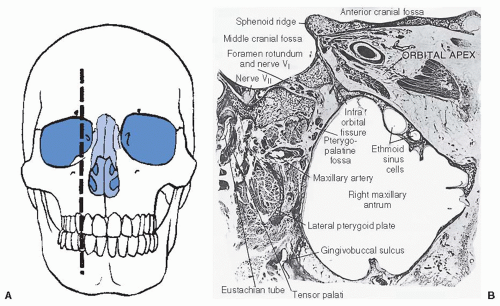 FIGURE 21-7. A: Sagittal section through the antrum and the apex of the orbit. B: The orbital apex communicates with the pterygopalatine fossa by way of the infraorbital fissure. Extension of antral tumor through the posterior wall provides access to the middle cranial fossa along the cranial nerves and the vascular foramina. Source: From Bridger MWM, van Nostrand AWP. The nose and paranasal sinuses—applied surgical anatomy: a histologic study of whole organ sections in three planes. J Otolaryngol. 1978;7(suppl 6):1-30, with permission. |
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


