Cancer of the larynx represents about 0.8% of the total cancer risk in 2010 and is one of the most common head and neck cancers.
1 In 2010 in the United States, there were approximately 12,720 new cases of cancer of the larynx (10,110 men and 2,610 women) and about 3,740 deaths from laryngeal cancer.
1 Based on 1992 to 1997 US data at diagnosis, about 51% of the cases remain localized, 29% have regional spread, and 15% have distant metastases.
2 Cancer of the larynx is strongly related to cigarette smoking. The risk of tobacco-related cancers of the upper alimentary and respiratory tracts declines among ex-smokers after 5 years and is said to approach the risk of nonsmokers after 10 years of abstention.
3 The role of alcohol in inducing laryngeal cancer remains unclear.
4 Some evidence exists that heavy marijuana smoking may be associated with laryngeal cancer in young patients. The ratio of glottic to supraglottic carcinoma is approximately 3:1.
ANATOMY
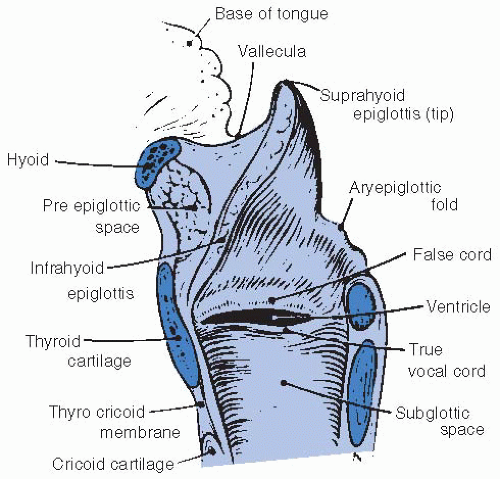
The larynx is divided into the supraglottic, glottic, and subglottic regions. The supraglottic larynx consists of the epiglottis, the false vocal cords, the ventricles, the aryepiglottic folds, and the arytenoids. The glottis includes the true vocal cords and the anterior commissure. The subglottis is located below the vocal cords (
Figs. 18-1 and
18-2).
5The lateral line of demarcation between the glottis and supraglottis is the apex of the ventricle. The demarcation between the glottis and subglottis is ill defined, but the subglottis is considered to begin 5 mm below the free margin of the vocal cord and to end at the inferior border of the cricoid cartilage.
The vocal cords vary from 3 to 5 mm in thickness and terminate posteriorly with their attachment to the vocal process. The mucosa between the arytenoids is called the posterior commissure.
The outside shell of the larynx is formed by the hyoid bone, thyroid cartilage, and cricoid cartilage; the cricoid cartilage is the only complete ring. The more mobile interior framework is composed of the heart-shaped epiglottis and the arytenoid, corniculate, and cuneiform cartilages. The corniculate and cuneiform cartilages produce small, rounded bulges at the posterior end of each aryepiglottic fold.
The thyroid and cricoid cartilages and a portion of the arytenoid cartilage are hyaline cartilage and may partially ossify with age, particularly in men. The epiglottis is elastic cartilage; ossification does not occur, and even focal calcification is rare.
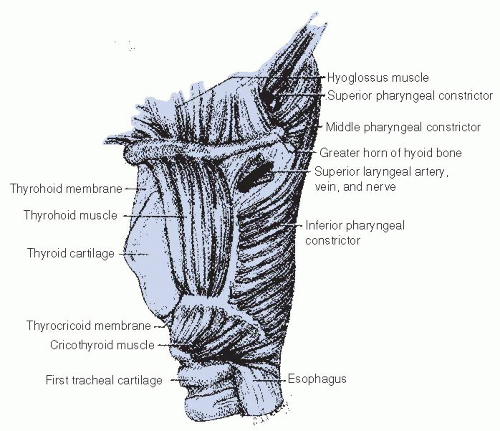
6The external laryngeal framework is linked together by the thyrohyoid, cricothyroid, and cricotracheal ligaments or membranes (
Figs. 18-3 and
18-4).
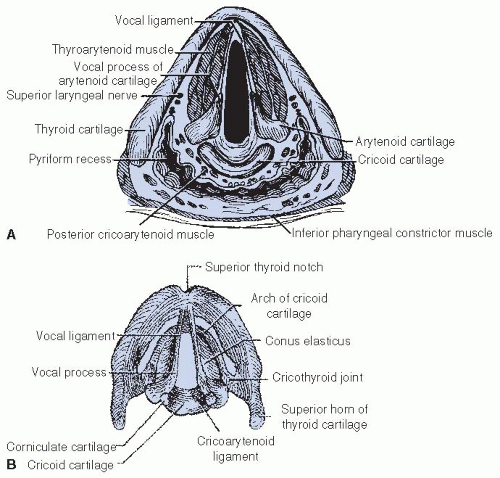
5The epiglottis is joined superiorly to the hyoid bone by the hyoepiglottic ligament. The epiglottis is attached to the thyroid cartilage by the thyroepiglottic ligament at a point just below the thyroid notch and above the anterior commissure. The arrangement of the ligaments that connect the cricoid and arytenoid cartilages and form the vocal ligaments, which are part of the true vocal cords, is shown in
Figure 18-2B. The conus elasticus (cricovocal ligament) is the lower portion of the elastic membrane that connects the inferior framework. It connects the upper surface of the cricoid, the vocal process of the arytenoid, and the lower thyroid cartilage; its free border is thickened into the vocal ligament.
The vocal ligaments and muscles attach to the vocal process of the arytenoid posteriorly and the thyroid cartilage anteriorly. The intrinsic muscles of the larynx, which primarily control the movement of the cords, are presented in
Figures 18-2 and
18-3.
5 The extrinsic muscles are concerned primarily with swallowing. The cricothyroid muscle produces tension and elongation of the vocal cords and is innervated by the superior laryngeal nerve (
Fig. 18-4).
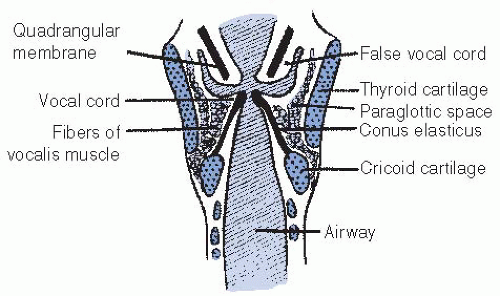
5The preepiglottic and paraglottic fat spaces are, for practical purposes, one continuous space lying between the external framework of the thyroid cartilage and hyoid bone and the inner framework of the epiglottis and intrinsic muscles. Lam and Wong
7 showed that the thin, membranous septa located between the paraglottic and preepiglottic space are capable of holding a tumor in check to a limited degree. The space is traversed by blood vessels, lymphatic vessels, and nerves. Because few capillary lymphatics arise in this area, invasion of the fat space should only indirectly be associated with lymph node metastases. The fat space is limited by the conus elasticus inferiorly, the thyroid ala, the thyrohyoid membrane, the hyoid bone anterolaterally, the hyoepiglottic ligament superiorly, and the fascia of the intrinsic muscles on the medial side. Posteriorly, it is adjacent to the anterior wall of the pyriform sinus.
The laryngeal surface of the epiglottis and the free margin of the vocal cords are squamous epithelium, and the remainder is usually pseudostratified ciliated columnar epithelium. Beneath the epithelium of the free edge of the vocal cord is the lamina propria, which can be divided into three layers. There is no true submucosal layer along the free margin of the vocal fold.
8 The laryngeal arteries are branches of the superior and inferior thyroid arteries.
The intrinsic muscles of the larynx are innervated by the recurrent laryngeal nerve. The cricothyroid muscle, an intrinsic muscle responsible for tensing the vocal cords, is supplied by a branch of the superior laryngeal nerve. Isolated damage to this nerve causes a bowing of the true vocal cord; it continues to be mobile, but the voice may become hoarse.
The supraglottic structures have a rich capillary lymphatic plexus. The trunks pass through the preepiglottic space and the thyrohyoid membrane and terminate mainly in the subdigastric lymph nodes (level 2); a few drain to the middle internal jugular chain lymph nodes (level 3). There are essentially no capillary lymphatics of the true vocal cords. As a result, lymphatic spread from glottic cancer occurs only if tumor extends to supraglottic or subglottic areas. The subglottic area has relatively few capillary lymphatics. The lymphatic trunks pass through the cricothyroid membrane to the pretracheal (Delphian) lymph nodes in the region of the thyroid isthmus. The subglottic area also drains posteriorly through the cricotracheal membrane, with some trunks going to the paratracheal lymph nodes and others continuing to the inferior jugular chain (level 4).
PATHOLOGY AND PATTERNS OF SPREAD
Pathology
Nearly all malignant tumors of the larynx arise from the surface epithelium and therefore are squamous cell carcinoma or one of its variants. Carcinoma in situ occurs frequently on the vocal cords. Differentiating among dysplasia, carcinoma in situ, squamous cell carcinoma with microinvasion, and true invasive carcinoma is a problem that the pathologist and the clinician frequently confront. Most vocal cord carcinomas are well differentiated or moderately well differentiated. In a few cases, an apparent carcinoma and sarcoma occur together, but most of these are actually a spindle-cell carcinoma or so-called pseudosarcoma (i.e., squamous cell carcinoma with a spindle-cell stromal reaction). Verrucous carcinoma occurs in 1% to 2% of patients with carcinoma of the vocal cord. The histologic diagnosis is difficult and must correlate with the gross appearance of the lesion.
Small cell neuroendocrine carcinoma is rarely diagnosed in the supraglottic larynx, but it should be recognized because of its biologic potential for rapid growth, early dissemination, and responsiveness to chemotherapy. Minor salivary gland tumors arise from the mucous glands in the supraglottic and subglottic larynx, but they are rare.
9 Even more rare are chemodectoma, carcinoid, soft tissue sarcoma, malignant lymphoma, or plasmacytoma. Benign chondromas and osteochondromas are reported, but their malignant counterparts are rare.
Local Spread
Although supraglottic and glottic lesions tend to remain confined to their original compartments, there is no anatomic barrier to growth from one area to the next. Glottic lesions tend to be slow growing, but as they increase in size, they extend to the supraglottic and subglottic areas. Supraglottic lesions do not often start near the vocal cords. Involvement of the cords on their external epithelial surface is a late phenomenon, but submucosal extension by way of the paraglottic area occurs earlier.
The fat space is an important avenue of submucosal tumor spread for infrahyoid epiglottis, false cord, and true vocal cord lesions. As the false cord and the true vocal cord lesions penetrate anteriorly and laterally, they encounter the tough perichondrium
of the thyroid cartilage and may eventually be shunted by the conus elasticus (lateral cricothyroid membrane) out of the larynx via the cricothyroid space. Thyroid cartilage invasion usually occurs in the ossified section of the cartilage, commonly in the region of the anterior commissure tendon or the junction of the anterior one-fourth and the posterior three-fourths of the thyroid lamina.
10Fixation of the vocal cord from laryngeal cancer is usually caused by invasion or destruction of the vocal cord musculature, invasion of the cricoarytenoid muscle or joint, or, rarely, invasion of the recurrent laryngeal nerve. Perineural spread is uncommon.
Supraglottic Larynx
Suprahyoid Epiglottis. A lesion of the suprahyoid epiglottis may produce a huge exophytic mass with little tendency to destroy cartilage or spread to adjacent structures. Other lesions may infiltrate the tip and destroy cartilage. The destructive lesions tend to invade the vallecula and preepiglottic space, the lateral pharyngeal walls, and the remainder of the supraglottic larynx.
Infrahyoid Epiglottis. Lesions of the infrahyoid epiglottis tend to produce irregular tumor nodules and simultaneously invade the porous epiglottic cartilage and thyroepiglottic ligament into the preepiglottic fat space and extend toward the vallecula and base of the tongue. The thick hyoepiglottic ligament is an effective tumor barrier. However, the tumor may present in the vallecula and base of tongue without involving the suprahyoid epiglottis.
Lesions of the infrahyoid epiglottis grow circumferentially to involve the false cords, aryepiglottic folds, medial wall of the pyriform sinus, and the pharyngoepiglottic fold. Invasion of the anterior commissure and cords and anterior subglottic extension usually occur only in advanced lesions. Infrahyoid epiglottic lesions that extend onto or below the vocal cords are at a high risk for thyroid cartilage invasion, even if the cords are mobile.
11False Cord. Early false cord carcinomas, which are usually submucosal with little exophytic component, are difficult to delineate accurately. They involve the paraglottic fat space early in their development and may spread a considerable distance beneath the mucosa without producing physical signs. These carcinomas extend to the perichondrium of the thyroid cartilage quite early, but cartilage invasion is a late phenomenon. Extension to the lower portion of the infrahyoid epiglottis and invasion of the preepiglottic space are common. Submucosal extension involves the true vocal cord, which may appear normal. Vocal cord invasion is often associated with thyroid cartilage invasion. Submucosal extension to the medial wall of the pyriform sinus occurs early.
Aryepiglottic Fold/Arytenoid. Early lesions of the aryepiglottic fold/arytenoid are usually exophytic. It may be difficult to decide whether the lesion started on the medial wall of the pyriform sinus or on the aryepiglottic fold. As the lesions enlarge, they extend to adjacent sites and eventually cause fixation of the larynx, which is usually a result of involvement of the cricoarytenoid muscle or joint or, rarely, invasion of the recurrent laryngeal nerve. Computed tomography (CT) may distinguish the cause of fixation. Advanced lesions invade the thyroid, the epiglottic, and the cricoid cartilages and eventually invade the pyriform sinus and postcricoid area.
Glottic Larynx
Most lesions of the true vocal cord begin on the free margin and upper surface of the cord. When diagnosed, about two-thirds are confined to the cords, usually one cord. The anterior portion of the cord is the most common site. Anterior commissure involvement, which is common, occurs when no tumor-free cord can be seen anteriorly. Small lesions isolated to the anterior commissure account for only 1% to 2% of cases. Extension to the posterior commissure is uncommon, occurring only in advanced lesions.
Tumors at the anterior commissure may extend anteriorly via the anterior commissure tendon (Broyles’ ligament)
12 into the thyroid cartilage. Kirchner,
11 using whole organ sections, showed that such extension is unusual unless the tumor extends off the vocal cord onto the base of the infrahyoid epiglottis and suggested that the tendon serves as more of a barrier than an avenue of tumor spread. Early subglottic extension is also associated with involvement of the anterior commissure, and tumor may grow through the cricothyroid membrane.
Lesions that arise on the posterior half of the vocal cord tend to extend along the submucosa toward the medial side of the vocal process and invade the cricoarytenoid joint and posterior commissure; this spread is difficult to appreciate by clinical examination.
Subglottic extension may occur by simple mucosal surface growth, but it more commonly occurs by submucosal penetration beneath the conus elasticus. One centimeter of subglottic extension anteriorly or 4 to 5 mm of subglottic extension posteriorly brings the border of the tumor to the upper margin of the cricoid, exceeding the anatomic limits for a conventional hemilaryngectomy. Lesions may spread beneath the epithelium along the length of the vocal cord within Reinke’s space.
13 As vocal cord lesions enlarge, they extend to the false cord, vocal process of the arytenoid, and subglottic region. Infiltrative lesions invade the vocal ligament and muscle and eventually reach the paraglottic space and the perichondrium of the thyroid cartilage. Advanced glottic lesions eventually penetrate through the thyroid cartilage or via the cricothyroid space to enter the neck, where they may invade the thyroid gland. Lesions involving the anterior commissure often exit the larynx via the cricothyroid space after they extend subglottically.
13A fixed cord that is associated with a lesion having <1 cm of subglottic extension and no false cord involvement does not ordinarily indicate invasion of the thyroid cartilage.
11 If the false cord is also involved, cartilage invasion is more likely.
Subglottic Larynx
Subglottic cancers are rare. Most involve the inferior surface of the vocal cords by the time they are diagnosed, so it is difficult to know whether the tumor started on the undersurface of the vocal cord or in the subglottis. Because early diagnosis is uncommon, most lesions are bilateral or circumferential at discovery. They involve the cricoid cartilages in the early stage because there is no intervening muscle layer. Partial or complete fixation of one or both cords is common; misdiagnosis or diagnostic delay is frequent.
Lymphatic Spread
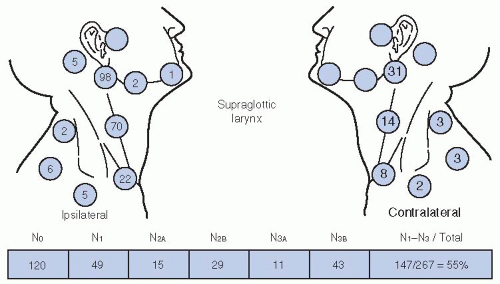
The location and stage of neck nodes detected on admission for previously untreated patients with squamous cell carcinoma of the supraglottic larynx are given in
Figure 18-5.
14 The disease spreads mainly to the subdigastric nodes (level 2). The submandibular nodes (level 1b) are rarely involved, and there is only a small risk of spinal accessory lymph node (level 5) involvement. The incidence of clinically positive nodes is 55% at the time of diagnosis; 16% are bilateral.
14 Elective neck dissection shows pathologically positive nodes in 16% of cases; observation of initially node-negative necks eventually identifies the appearance of positive nodes in 33% of cases.
15,16 Spread to the pyriform sinus, the vallecula, and the base of the tongue increases the risk of
lymph node metastases. The risk of late-appearing contralateral lymph node metastasis is 37% if the ipsilateral neck is pathologically positive, but the risk is unrelated to whether the nodes in the ipsilateral neck were palpable before neck dissection.
In carcinoma of the vocal cord, the incidence of clinically positive lymph nodes at diagnosis approaches zero for T1 lesions and 1.7% for T2 lesions.
17 The incidence of neck metastases increases to 20% to 30% for T3 and T4 lesions. Supraglottic spread is associated with metastasis to the jugulodigastric nodes. Anterior commissure and anterior subglottic invasion are associated with involvement of the midline pretracheal lymph nodes (Delphian nodes).
Lederman
18 reported a 10% incidence of positive lymph nodes in 73 patients with subglottic carcinoma.
CLINICAL PRESENTATION
Carcinoma arising on the true vocal cords produces hoarseness at a very early stage. Sore throat, ear pain, pain localized to the thyroid cartilage, and airway obstruction are features of advanced lesions.
Hoarseness is not a prominent symptom of cancer of the supraglottic larynx until the lesion becomes quite extensive. Pain on swallowing, usually mild, is the most frequent initial symptom, often described as a sore throat. Some patients report a sensation of a “lump in the throat.” Pain is referred to the ear by way of the vagus nerve and auricular nerve of Arnold. A mass in the neck may be the first sign of a supraglottic cancer. Late symptoms include weight loss, foul breath, dysphagia, and aspiration.
DIAGNOSTIC EVALUATION AND CLINICAL STAGING
Physical Examination
Flexible fiberoptic endoscopes are now used routinely as a complement to the laryngeal mirror examination. The mirror gives a larger image of the larynx or the hypopharynx than that obtained by direct laryngoscopy or fiberoptic endoscopy. The mirror often provides the best view of the posterior pharyngeal wall. The flexible fiberoptic laryngoscope is inserted through the nose and is useful in more difficult cases.
Determination of the mobility of the vocal cords frequently requires multiple examinations because the subtle distinctions between mobile, partially fixed, and fixed cords are often challenging, apparently changing from examination to examination. A cord that appeared mobile to the surgeon before direct laryngoscopy may exhibit impaired motion or even fixation after biopsy. Videostroboscopy is particularly useful for assessing vocal cord mobility.
Ulceration of the infrahyoid epiglottis or fullness of the vallecula is an indirect sign of preepiglottic space invasion. Palpation of diffuse, firm fullness above the thyroid notch with widening of the space between the hyoid and the thyroid cartilage signifies invasion of the preepiglottic space. The preepiglottic fat space is a low-density area on the CT scan, and changes resulting from tumor invasion are easily seen.
Postcricoid extension may be suspected when the laryngeal click disappears on physical examination. Postcricoid tumor may cause the thyroid cartilage to protrude anteriorly, producing a fullness of the neck.
Invasion of the thyroid cartilage remains a difficult clinical diagnosis. Localized pain or tenderness to palpation or a small bulge over one ala of the thyroid cartilage is suggestive.
Radiographic Studies
Contrast-enhanced CT scan is the method of choice for studying the larynx. The CT scan should be performed before biopsy so that abnormalities that may be caused by the biopsy are not confused with tumor. CT is preferred to magnetic resonance imaging (MRI) because the longer scanning time for MRI may result in motion artifact.
19 CT slices 1 to 2 mm thick are obtained at 1 to 2 mm intervals through the larynx and at 3 mm intervals for the remainder of the study. The gantry is angled so that the scan slices are parallel to the plane of the true vocal cords. It is also necessary to obtain a CT scan of the entire neck to detect positive, nonpalpable lymph nodes. Positive retropharyngeal nodes
may be present at diagnosis in patients with laryngeal cancer who have advanced neck disease.
20 Retropharyngeal adenopathy is often not apparent on physical examination but is usually apparent on the CT scan.
Contrast enhancement helps to outline the blood vessels and thyroid gland. The tumor often enhances, probably because of reactive inflammatory changes. In addition to CT, MRI may be obtained to define subtle exolaryngeal spread or early cartilage destruction. The value of MRI for detecting early cartilage destruction is open to speculation. Sagittal MRI may be useful in detecting early invasion of the base of the tongue.
Positron emission tomography (PET) is not routinely obtained. It may be useful to evaluate a questionable finding on CT or MRI if that finding would alter the treatment plan. It may also be useful to determine whether or not distant metastases exist in a patient with advanced neck disease, particularly if it involves low neck below Ho’s line.
21
Glottic Larynx
Although the CT scan does not show minimal mucosal lesions, it is excellent for determining subglottic extension and extension anterior to the anterior commissure and is used in virtually all T1 and T2 lesions for these reasons alone. CT scanning is useful in the diagnosis of moderately advanced and advanced lesions; it is excellent for demonstrating extension outside the larynx into the soft tissues of the neck and has potential for determining thyroid or cricoid cartilage invasion, which tends to occur at the edges of the cartilage rather than on the faces. Early cartilage involvement is difficult to detect with axial scans, but it may be demonstrated by coronal or sagittal scanning techniques. If the low-density plane of the paraglottic space is intact, cartilage is probably not invaded by tumor. CT is also useful for evaluating the neck. Radiographically positive adenopathy may be appreciated that would otherwise be undetectable.
Supraglottic Larynx
The CT scan provides an excellent means for viewing the preepiglottic and paraglottic fat spaces. Soft tissue extension into the neck or base of the tongue also can be seen. The CT scan is also useful for determining extension to the subglottic areas and to evaluate the neck.
6
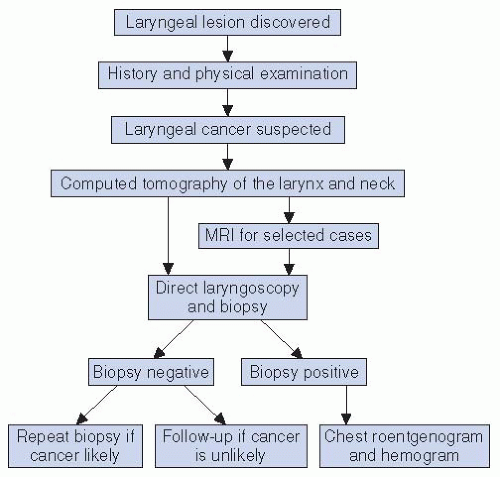
Direct Laryngoscopy
Diagnostic procedures for laryngeal cancer at the University of Florida are summarized in
Figure 18-6. A CT scan is usually performed, followed by direct laryngoscopy and biopsy. The ventricles, the subglottis, the apex of the pyriform sinus, and the postcricoid area must be carefully examined because these areas are not consistently seen by indirect examinations. Fiberoptic telescopes (0 degree and 30 degrees) are introduced through the laryngoscope for inspection of these areas. Endoscopic visualization facilitates the assessment of arytenoid fixation and involvement of the laryngeal ventricle, factors which must be considered before laryngeal preservation surgery is attempted. A generous biopsy specimen is taken from the obvious lesion; additional biopsies may be obtained from suspicious areas. In cases where the lesion is limited and superficial, directed biopsies that are guided by the surface appearance of the lesion may fail to detect foci of microinvasion, resulting in sampling error; thus, excisional biopsy should be considered whenever possible. Diffuse mucosal abnormalities suspicious for premalignancy should be endoscopically excised with the CO
2 laser or by using cold instrument dissection in lieu of crude vocal cord stripping to spare the superficial lamina propria, thereby optimizing postoperative voice quality.
Clinical Staging
The 2010 American Joint Committee on Cancer (AJCC) staging system for laryngeal primary cancer is listed in
Table 18.1.
22 T2 glottic cancers are stratified into those with normal (T2A) and impaired (T2B) vocal cord mobility. For lesions arising in the supraglottis, the sites of origin include the false cords, the aryepiglottic folds, the suprahyoid epiglottis, the infrahyoid epiglottis, the pharyngoepiglottic folds, and the arytenoids.
Only in the early T stages can one identify the specific site of origin with certainty. As the lesion enlarges, the site of origin is an educated guess based on the location of the greatest bulk of tumor. The major difference between the 1992 and 2010 staging systems is that a supraglottic cancer that invades the mucosa of the base of tongue and/or medial wall of the pyriform sinus can be staged as a T2 lesion. This has resulted in a reverse “Will Rogers effect” and negative stage migration such that the likelihood of local control for supraglottic cancer will likely be lower within each T stage while remaining the same overall. In contrast, invasion of the paraglottic space now upstages a T2 cancer to a T3. Parenthetically, we have evaluated the impact of paraglottic space invasion determined by pretreatment CT in a series of patients with T2 glottic cancers and found no significant adverse effect on local control after definitive radiotherapy (RT).
23 Additionally, T4 cancers have been stratified into T4A and T4B, which reflects the likelihood of achieving a complete resection.
TREATMENT SELECTION: VOCAL CORD CARCINOMA
Selection of Treatment Modality
In treating vocal cord carcinoma, the goal is cure with the best functional result and the least risk of a serious complication. Patients may be considered to be in an early group if the chance
of cure with larynx preservation is high, a moderately advanced group if the likelihood of local control is 60% to 70% but the chance of cure is still good, and an advanced group if the chance of cure is moderate and the likelihood of laryngeal preservation is relatively low. The early group may be treated initially by RT or, in selected cases, by partial laryngectomy. The moderately advanced group may be treated with either RT or partial laryngectomy with total laryngectomy reserved for relapse or by total laryngectomy with or without adjuvant postoperative RT. The obvious advantage of the former strategy, which we use at the University of Florida, is that there is a fairly good chance that the larynx will be preserved.
24 Although some patients may be rehabilitated with a tracheoesophageal puncture after laryngectomy, only about 20% of patients use this device long term and the majority use an electric larynx.
25 The advanced group is treated with total laryngectomy and neck dissection with or without adjuvant RT or by RT and adjuvant chemotherapy.
26 Data suggest that if patients whose tumors show a partial or complete response to two to three cycles of neoadjuvant chemotherapy are then given high-dose RT, the cure rates are comparable to those obtained with initial total laryngectomy.
27 Another less expensive and less toxic method to select patients likely to be cured by RT alone is to calculate the primary tumor volume on pretreatment CT or MR. Data indicate that primary tumor volume is inversely related to the probability of local control after irradiation.
28,29 Data indicate that whereas induction chemotherapy probably does not improve the likelihood of local-regional control and survival, concomitant chemotherapy and RT result in an improved possibility of cure compared with RT alone.
30,31,32 There is a subset of patients with high volume (>3.5 cc), unfavorable, advanced cancers who may be cured by chemoradiation but have a useless larynx and permanent tracheostomy and/or gastrostomy.
28 These patients are best treated with a total laryngectomy, neck dissection, and postoperative RT.
Carcinoma In Situ
Lesions diagnosed as carcinoma in situ may sometimes be controlled by stripping the cord. However, it is difficult to exclude the possibility of microinvasion on these specimens. Recurrence is frequent, and the cord may become thickened and the voice hoarse with repeated stripping. Localized carcinoma in situ can also be excised using the CO2 laser.
Early RT for carcinoma
in situ often means a better chance of preserving a good voice, especially since many patients with this diagnosis eventually receive this treatment.
33Many patients with a diagnosis of carcinoma in situ have obvious lesions that probably contain invasive carcinoma. We have often proceeded with RT rather than put the patient through a repeated biopsy procedure.
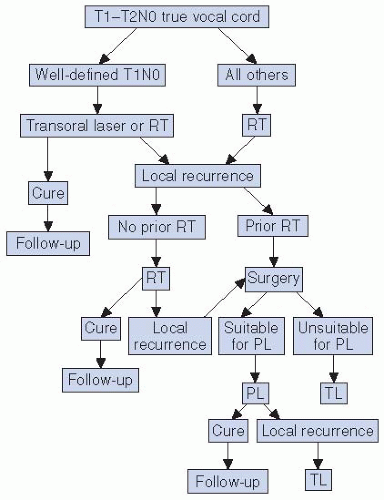
Early Vocal Cord Carcinoma
In most centers, RT is the initial treatment prescribed for T1 and T2 lesions, with surgery reserved for salvage after RT failure
34,35,36 (
Fig. 18-7). Although hemilaryngectomy or cordectomy produces comparable cure rates for selected T1 and T2 vocal cord lesions, RT is generally preferred.
34,37 Supracricoid laryngectomy, as reported by Laccourreye et al.,
38 is a procedure designed to remove moderate-sized cancers involving the supraglottic and the glottic larynx. The larynx may be removed with preservation of the cricoid and the arytenoid with its neurovascular innervation, the defect is closed by approximating the base of the tongue to the remaining larynx. The oncologic and functional results of this procedure in selected patients are reported to be excellent. Transoral laser excision also may provide high cure rates for select patients with small, well-defined lesions limited to the mid-third of one true cord.
39,40,41,42,43 A small subset of transoral laser surgeons successfully use this technique in moderately advanced cancers.
34 The major advantage of RT compared with partial laryngectomy is better quality of the voice. Partial laryngectomy finds its major use as salvage surgery in suitable cases after RT failure. Even if the patient has a local recurrence after salvage partial laryngectomy, there is a third chance with total laryngectomy, which may still be successful.
Verrucous lesions have the reputation of being unresponsive to RT and, in some instances, converting into invasive, often anaplastic, metastasizing lesions. Partial laryngectomy is recommended for early verrucous carcinoma of the glottis, but RT is recommended if the alternative is total laryngectomy. We have observed typical verrucous lesions that have disappeared with RT and not recurred. O’Sullivan and associates
44 also have made this observation. Additionally, a variety of tumors that recur after unsuccessful treatment (with surgery, RT, and/or chemotherapy) are more likely to exhibit more aggressive behavior.
Moderately Advanced Vocal Cord Cancer
Fixed-cord lesions (T3) may be subdivided into relatively favorable or unfavorable lesions. Patients with unfavorable lesions usually have extensive bilateral disease with a compromised airway and are considered to be in the advanced group. Patients with favorable T3 lesions have disease that is low volume (≤3.5 cc), confined mostly to one side of the larynx, have a good airway, and are reliable for follow-up. Some degree of supraglottic and subglottic extension usually exists. The extent of disease and tumor volume, in particular, are related to the likelihood of control after RT.
28The patient with a favorable lesion is advised of the alternatives of RT with surgical salvage or immediate total laryngectomy; the occasional patient may be suitable for a partial laryngectomy. Data suggest that the likelihood of local-regional control is better after some altered fractionation schedules compared with conventional once-daily RT.
32,45 Follow-up examinations are recommended every 4 to 6 weeks for the first year, every 6 to 8 weeks for the second year, every 3 months for the third year, every 6 months for the fourth and fifth years, and annually thereafter. The patient must understand that total laryngectomy may be recommended purely on clinical grounds without biopsy-proven recurrence and that the risk of laryngeal osteochondronecrosis is about 5%.
Evaluation of cord mobility after 50.4 Gy or at the end of RT has not been helpful in predicting local control.29 Some patients in whom the vocal cord remained fixed have had local tumor control of the disease for 2 years or longer after RT.
The major difficulty in using RT for the more advanced lesions is distinguishing radiation edema from local recurrence during follow-up examinations.
46 Progressive laryngeal edema, persistent throat pain, or fixation of a previously mobile vocal cord frequently signifies recurrent disease in the larynx, although a few patients with these findings remain disease free with long-term follow-up.
Partial laryngectomy has been used by a few surgeons in the treatment of well-lateralized fixed-cord lesions. A permanent tracheostomy is usually required because a portion of the cricoid is resected, but a useful voice may be retained.
47
Advanced Vocal Cord Carcinoma
Advanced lesions usually show extensive subglottic and supraglottic extension, bilateral glottic involvement, and invasion of the thyroid, cricoid, and/or arytenoid cartilages.
10,48 The airway is compromised, necessitating a tracheostomy at the time of direct laryngoscopy in approximately 30% of patients. Clinically positive lymph nodes are found in about 25% to 30% of patients.
The mainstay of treatment is total laryngectomy, with or without adjuvant RT. The most frequent sites of local failure after total laryngectomy are the tracheal stoma, the base of tongue, the neck lymph nodes, and/or soft tissues of the neck. If the neck is clinically negative before surgery and if postoperative RT is planned, neck dissection may be withheld and RT may be used to treat both sides of the neck. However, in practice, most surgeons prefer to perform elective bilateral selective (levels II-IV) neck dissections in conjunction with a total laryngectomy for T3N0 or T4N0 laryngeal cancer, even if postoperative RT is planned. If the lymph nodes are clinically positive, a therapeutic neck dissection is performed at the time of laryngectomy.
The indications for postoperative RT include close or positive margins, significant subglottic extension (1 cm or more), cartilage invasion, perineural invasion, endothelial-lined space invasion, extension of the primary tumor into the soft tissues of the neck, multiple positive neck nodes, extracapsular extension, and control of subclinical disease in the opposite neck.
49,50 Preoperative RT is indicated for patients who have fixed neck nodes, have had an emergency tracheotomy through tumor, or have direct extension of tumor involving the skin.
Definitive RT is prescribed for the patient who refuses total laryngectomy or is medically unsuitable for major surgery.
As previously stated, there is evidence that two to three cycles of induction chemotherapy followed by RT in patients obtaining at least a partial response may provide a moderate likelihood of larynx preservation without compromising cure.
27 Data suggest that concomitant chemotherapy and RT is more efficacious than RT alone or induction chemotherapy followed by RT.
30,31 The optimal combination of concomitant chemotherapy and irradiation is unclear.
32A randomized intergroup trial (RTOG 91-11) compared three treatment arms: Arm A, three cycles of induction cisplatin and fluorouracil followed by RT in complete and partial responders; Arm B, RT and concomitant cisplatin (100 mg/m
2 on days 1, 22, and 43 of RT); and Arm C, once-daily RT (70 Gy in 35 fractions over 7 weeks) alone.
30 Five hundred forty-seven patients were
randomized and followed for a median of 3.8 years; 518 patients were evaluable. The rates of larynx preservation were: Arm A, 72%; Arm B, 84%; and Arm C, 67%. The rates of larynx presentation were significantly improved for Arm B; there was no significant difference between Arm A and Arm C. The 5-year survival rates were similar for the three treatment groups: Arm A, 55%; Arm B, 54%; and Arm C, 56%. The likelihood of developing distant metastases was lower for the two groups of patients that received adjuvant chemotherapy.
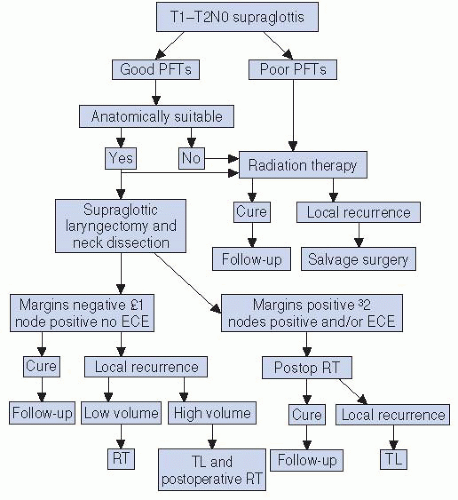
TREATMENT SELECTION: SUPRAGLOTTIC LARYNX CARCINOMA
Selection of Treatment Modality
Patients with supraglottic laryngeal carcinoma may be considered to be in an early or favorable group suitable for RT or conservation laryngectomy or an unfavorable group often requiring total laryngectomy (
Fig. 18-8).
Early and Moderately Advanced Supraglottic Lesions
Treatment of the primary lesion for the early group is by RT or supraglottic laryngectomy, with or without adjuvant RT.
51 Transoral laser excision is effective in experienced hands for selected lesions and is currently preferred to open approaches by many surgeons.
40 Total laryngectomy is rarely indicated as the initial treatment for this group of patients and is reserved for treatment failures.
RT and partial laryngectomy are highly successful modes of therapy for early lesions.
51 Approximately 50% of supraglottic laryngectomies performed at the University of Florida have been followed by postoperative RT because of neck disease and, less often, positive margins.
The decision to use RT or supraglottic laryngectomy depends on several factors including the anatomic extent of the tumor, medical condition of the patient, philosophy of the attending physician(s), and the inclination of the patient and the family. Overall, about 80% of patients are treated initially by RT. Approximately half of the patients seen in our clinic whose lesions are technically suitable for a supraglottic laryngectomy are not suitable for medical reasons (e.g., inadequate pulmonary status or other major medical problems); these patients are treated with RT.
Analysis of local control by anatomic site within the supraglottic larynx shows no obvious differences in local control by RT for similarly staged lesions. Invasion of the preepiglottic space is not a contraindication to supraglottic laryngectomy or RT. Primary tumor volume based on pretreatment CT is inversely related to local tumor control after RT.
28 A large, bulky (>6 cc) infiltrative lesion, especially one with extensive preepiglottic space invasion, is a common reason to select supraglottic laryngectomy.
The status of the neck often determines the selection of treatment of the primary lesion. Patients with clinically negative neck nodes have a high risk for occult neck disease and may be treated by RT or supraglottic laryngectomy and bilateral selective neck dissections (levels II-IV).
If a patient has an early-stage primary lesion but advanced neck disease (N2b or N3), combined treatment is frequently necessary to control the neck disease.
26 In these cases, the primary lesion is usually treated by definitive RT, with surgery added to the treatment of the involved neck site(s). If the same patient were treated with supraglottic laryngectomy, neck dissection, and postoperative RT, the portals would unnecessarily cover the primary site and the neck. If the patient has early, resectable neck disease (N1 or N2a) and surgery is elected for the primary site, postoperative RT is added only because of unexpected findings (e.g., positive margins, multiple positive nodes, or extracapsular extension). Patients who have positive margins at the primary site after a partial laryngectomy should not have been treated surgically; the postoperative RT dose to the remaining larynx is likely to result in major complications requiring a permanent tracheostomy and/or gastrostomy. The usual indurations for postoperative RT are related to neck disease. The remaining larynx is treated to 55.8 Gy at 1.8 Gy per fraction and the involved neck is boosted to a higher dose as needed.
52