More than 3.5 million new skin cancers are diagnosed every year. Although melanoma represents <5% of the cases, it is responsible for >75% of skin cancer-related deaths.1 Thus, melanoma is the most aggressive form of skin cancer, and it is likely to be an increasingly prevalent problem in the future. An estimated 70,230 patients will be diagnosed with melanoma, and 8,790 will die from this disease, in the United States in 2012.2 Currently, the lifetime risk of being diagnosed with melanoma is 1 in 37 for men and 1 in 55 for women. Concerningly, the incidence of melanoma has increased dramatically over the last several decades, with an increase of >200% in the age-adjusted incidence from 1975 to 2008.3,4,5,6,7,8 The rise in incidence has been detected across all age groups and primary tumor thicknesses. The mortality rate has also increased approximately 60% over time, primarily due to increased mortality in patients >65 years of age, particularly among men.3,7,8 However, many patients who die from melanoma are otherwise young and healthy, leading to melanoma being among the cancers with the highest lifeyears lost per fatality.9,10
Although melanoma is a highly aggressive cancer, patients can be cured of this disease if they are diagnosed early and managed appropriately. Carefully conducted studies over the last 20 years have defined the clinical and pathological criteria that define patient prognosis and guide current patient management.11,12,13 Historically, melanomas have been grouped based on clinical and pathological features. However, recent discoveries about the molecular biology of melanoma have provided key insights into the molecular heterogeneity of this disease and are rapidly leading to new therapeutic approaches and improved clinical outcomes.14 This chapter will review the existing standards for melanoma diagnosis and treatment and will discuss the recent advances in research and their implications for future patient management.
ANATOMY
Melanomas of the head and neck most commonly present on the face, which corresponds to the area that has received the highest lifetime cumulative dosages of ultraviolet light. The scalp and ears are the next most common sites of presentation, followed by the skin of the neck. Due to the substantial cosmetic considerations associated with facial surgery, it is imperative that the operating surgeon has an understanding of the anatomic subunits of the facial structures and of lines of normal skin tension. On the nasal cavity, these include the dorsum, the nasal sidewalls, the nasal ala, the columella, and the tip. On the ears, these include the helix, the conchal bowl, the antihelix, and the lobule. On the eyes, these include the superior orbital rim, the inferior orbital rim, the medial canthal region, and the lateral canthal region. Placement of surgical incisions within the lines of normal skin tension will allow surgical reconstruction to proceed in a cosmetically appealing manner.
Of utmost importance in the management of head and neck melanoma is a concrete understanding of the surgical anatomy of the lymphatics, as the status of the regional nodes has the most impact on survival. For sentinel lymph node biopsy (SLNB), the identification of lymph nodes in the head and neck may be challenging due to their relationship to the cranial nerves. In particular, the lymphatics of the parotid gland may be superficial to the gland or may be embedded deep within the substance of the soft tissue, and surgical exploration for sentinel lymph nodes in this basin may place the facial nerve at risk for injury. Lymphatic drainage of regions such as the nasal skin, the lip, and the midface frequently drain to more than one nodal basin and may also drain in bilateral or contralateral directions.15 Commonly, the facial lymph nodes that traverse the facial artery and vein are sites of SLN, and removal of these places the marginal mandibular branch of the facial nerve at risk.
Lesions of the scalp that are anterior to a line drawn along the coronal plane through the tragus oftentimes will drain to the parotid, the submental, or the anterior cervical lymph nodes.16 Alternatively, melanomas that are posterior to this line will most often drain to either the suboccipital, the retroauricular, or the posterior triangle cervical lymphatics.17 The removal of nodes that map to the posterior triangle places the spinal accessory nerve at risk for injury during the surgical excision. Thus, a precise understanding of the anatomy of the cervical lymphatics and of the cranial nerves is of critical necessity for surgeons managing patients with melanoma of the head and neck. Further elaboration of the anatomy of the cervical lymphatics may be found in other chapters in this text.
RISK FACTORS
Improved awareness and screening are likely partially responsible for the marked increase in the incidence of melanoma over the last few decades. However, there is strong evidence that increased exposure to ultraviolet radiation (UVR) also plays a role.18 Multiple studies support a causative role for UVR in cutaneous melanoma, including migration and epidemiologic studies.3 A history of sunburns from natural UVR and the use of tanning beds (artificial UVR) are risk factors for melanoma, and public surveys have reported increasing prevalence of both behaviors among US adults.19 Interestingly, while intermittent sun damage/exposure has consistently been identified as a positive risk factor, some studies suggest that chronic sun exposure is associated with a decrease in the risk of melanoma.20 Other risk factors for cutaneous melanoma include a positive family history, multiple nevi, dysplastic nevi, freckled or fair skin, blue or green eye color, and red hair color.21,22 The phenotype of fair skin, freckling, and red hair has been linked to polymorphisms in the MC1R gene, which encodes the melanocortin-1 receptor.23 The polymorphisms in MC1R cause decreased signaling through the receptor, which ultimately results in decreased melanin production. The primary function of melanin is to absorb UVR, thus protecting cellular DNA from its damaging effects. Germline polymorphisms in other genes involved in melanin synthesis (TYR, TYRP1) have also been linked to an increased melanoma risk and further implicate the role of UVR in this disease.23
Approximately 10% of melanomas are familial (>3 affected individuals). Familial melanomas are associated with a very early age of onset, frequently in areas without UVR exposure. The most common genetic feature in these families is germline deletion or inactivating mutation of the CDKN2A gene on chromosome 9.23 Due to alternative splicing, CDKN2A is transcribed into two different proteins (p16INK4A and p14ARF) which regulate cell cycle progression and cause cell cycle arrest in response to DNA damage. Inactivation of CDKN2A is detected in approximately 40% of melanoma-prone families. The critical role of DNA damage is also implicated by the identification of melanoma-prone families with germline mutations in the CDK4 gene.23 The detected genetic alterations result in a mutant CDK4 protein that is resistant to inhibition by pl6INK4A and thus recapitulate loss of CDKN2A. Polymorphisms in a number of other genes involved in DNA repair have also been associated with increased risk of melanoma.24
PATHOLOGY
Developmentally, melanocytes arise from the neural crest. The cells migrate most commonly to the epidermis of the skin, but they can also be found in the meninges lining the brain, the uveal tract of the eye, and the ectodermal mucosa. Melanomas can arise from each of these sites and are thereby clinically classified as cutaneous, primary meningeal, uveal, and mucosal melanomas. Cutaneous melanomas, which are by far the most common subtype, have been further subdivided into categories defined by a combination of pathological and clinical features. The majority of cutaneous melanomas fall into one of the following subtypes: superficial spreading melanoma (SSM), nodular melanoma (NM), lentigo maligna melanoma (LMM), and acral lentiginous melanoma (ALM). A rarer but clinically relevant subtype in the head and neck is desmoplastic melanoma (DM).
Superficial spreading melanomas, the most common subtype (˜70%) of cutaneous melanomas, generally arise on any skin with intermittent sun exposure. Nodular melanomas (˜15%) are characterized by vertical growth without a prior radial growth phase. Nodular melanomas are often highly aggressive and clinically appear as raised nodules. Lentigo maligna melanomas (˜10%) appear as flat brown macules, often with hypopigmented areas. Lentigo maligna melanomas are associated with chronic sun exposure and are typically located on the head, neck, and arms. Acral lentiginous melanoma (˜5%) is the least common subtype among Caucasians, but represents 30% to 70% of the melanomas diagnosed in African Americans and Hispanics. Acral lentiginous melanomas occur on the palms or soles, or underneath the nail plate, where exposure to UVR is relatively limited. DMs occur in areas with chronic sun exposure, particularly of the head and neck. DM are usually detected in elderly patients and are highly invasive, often presenting as lesions with significant (>5 mm) thickness. DMs often invade along neural tracks, which can result in significant symptomatology.
MOLECULAR BIOLOGY
A variety of studies have demonstrated that there are significant molecular differences between the melanoma subtypes. Wholegenome copy number analyses have demonstrated that cutaneous, acral, and mucosal melanomas are characterized by distinct patterns of chromosomal gain and loss.25 Furthermore, cutaneous melanomas with and without evidence of chronic sun damage (CSD) show distinct patterns of DNA copy number changes; tumors with evidence of CSD appear relatively similar to acral and mucosal melanomas. Uveal melanomas show a pattern of chromosomal aberrations that are distinct from the cutaneous and mucosal melanomas and are characterized by a high prevalence of isosomy of chromosome 3, which is associated with poor clinical outcomes.26,27
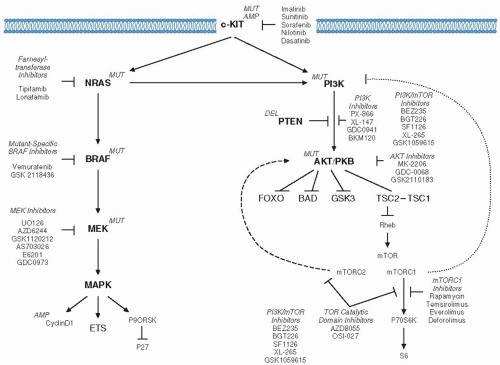
In addition to differences in the pattern of chromosomal changes, melanoma subtypes are characterized by differences in the prevalence of somatic mutations, a number of which are emerging as both prognostic markers and therapeutic targets (Table 24.1).14,28,29 The most common somatic event in melanoma is alteration of the BRAF gene.30BRAF encodes serine-threonine kinase that is a key component of the RAS-RAF-MEK-ERK signaling pathway (Fig. 24-1). More than 90% of the alterations in BRAF that are detected in melanoma are missense mutations that affects the valine residue at position 600.31,32 The most common mutation (˜75% of BRAF mutations) results in substitution of a glutamic acid (V600E), which increases the catalytic activity of the BRAF protein >100-fold.33 Melanoma cell lines with activating BRAF mutations demonstrate constitutive activation of MEK and ERK signaling and functionally depend on this pathway for growth and survival.34 Mutation of NRAS, which also results in hyperactivation of MEK and ERK, is the second most common somatic event in melanoma and thus reinforces the critical role of the RAS-RAF-MEK-ERK pathway in this disease.32
Studies of the clinical correlates of BRAF mutations have found positive associations with both younger age and a lack of CSD.35,36,37 Although activating BRAF mutations are detected in 45% to 50% of cutaneous melanomas without CSD, the rate is lower (10%-30%) in tumors with histologic evidence of sun damage (i.e., solar elastosis).25,38BRAF mutations are also relatively rare in acral (10%-15%), mucosal (5%), and uveal melanomas (<1%).25,32,39NRAS mutations are associated with thicker primary tumors and shorter relapse-free survival (RFS) from initial melanoma diagnosis.35,40NRAS mutations appear to have a similar prevalence of approximately 20% in cutaneous melanomas with and without CSD, but a lower prevalence in acral (15%), mucosal (10%), and uveal (<1%) melanomas.25,32
TABLE 24.1 Melanoma Subtypes: Genetic Mutations
Cutaneous
Acral
Mucosal
Uveal
Clinical features
Most common subtype
Involving skin on palms, soles, or nailbeds
Mucosal surfaces of head and neck, gastrointestinal, or genitourinary tract
Arise from melanocytes in the ciliary tract of the eye
Source: Adapted from Davies MA, Gershenwald JE. Targeted therapy for melanoma: a primer. Surg Onc Clin NAm. 2011;20:165-180, with permission from Elsevier.
FIGURE 24-1. Molecular biology of melanoma. The figure illustrates pathways that are affected by somatic mutations in melanoma. MUT, activating mutation; AMP, gene amplification; DEL, loss of function.
Source: Adapted from Davies MA, Gershenwald JE. Targeted therapy for melanoma: a primer. Surg Onc Clin NAm. 2011;20:165-180, with permission from Elsevier.
The relative paucity of activating BRAF mutations in CSDcutaneous, acral, and mucosal melanomas led to interrogations of regions of DNA copy number gain for additional oncogenic drivers in these subtypes. These studies resulted in the identification of frequent abnormalities in the KIT gene in these subtypes.41 The KIT gene encodes a receptor tyrosine kinase that is also frequently activated genetically in gastrointestinal stromal tumors (GIST), testicular seminomas, and certain types of leukemia.42 In addition to amplifications, initial studies identified somatic mutations in the KIT gene in melanomas. Overall, KIT mutation or amplification were identified in 36% of acral and 39% of mucosal melanomas. KIT alterations in cutaneous melanomas without CSD have consistently been reported to be quite rare (≤1%), but variable results (2%-28%) have been reported for cutaneous melanomas with CSD.38,41
A variety of other somatic alterations have been identified in melanoma (Fig. 24-1).14,29 Inactivating mutations and deletions of PTEN, a negative regulator of the PI3K-AKT signaling pathway, have been identified in 10% to 30% of melanomas.43 Loss of PTEN expression in the absence of detectable abnormalities in the PTEN gene has also been reported, consistent with epigenetic regulation of the gene.44,45 Genetic inactivation of PTEN is mutually exclusive with the presence of activating NRAS mutations in melanoma, but frequently occurs in tumors and cell lines that have activating BRAF mutations.46,47 Although BRAF, NRAS, and KIT mutations are very rare in uveal melanomas, these tumors frequently have activating mutations in GNAq (45%) or GNA11 (35%).48,49,50 Both GNAq and GNA11 encode regulatory subunits of G-protein coupled receptors, which may activate many of the same pathways affected by the mutations that are common in other melanoma subtypes. Uveal melanomas also frequently have inactivating somatic mutations of the BAP1 gene, which is located on chromosome 3, and may function as a tumor suppressor in this melanoma subtype.51
PATTERNS OF SPREAD
The clinical course of cutaneous melanoma is highly variable. Cutaneous melanomas can spread locally through dermal lymphatic channels to form cutaneous satellite lesions (within 2 cm of the primary lesion), as well as in-transit lesions along the course of the draining lymphatics. More commonly, initial tumor progression presents as metastasis to draining regional lymph nodes. Distant metastases generally are diagnosed after the development of regional involvement, although some patients have their first relapse at distant sites. In addition, approximately 5% of melanoma patients present with metastasis(es) with no detectable primary tumor.52 Melanoma can metastasize to virtually any distant organ, including skin, lymph node, lung, liver, GI tract, and bone, among others. One of the most common sites of distant metastasis is the brain. Approximately 60% of patients with distant metastases will develop brain involvement at some time during the course of their disease, and up to 80% of metastatic melanoma patients have evidence of brain involvement in autopsy series.53,54
Similar to cutaneous melanoma, mucosal melanomas tend to spread initially to regional lymph nodes and then subsequently to distant sites. In contrast to cutaneous and mucosal melanomas, uveal melanomas spread almost uniquely hematogenously, and thus lymph node involvement is quite rare. However, almost all uveal melanoma patients with distant disease have liver involvement (95%). Some patients also develop metastases to the lungs (25%), bone (15%), and skin (10%), but uveal melanomas almost never metastasize to the brain.55
CLINICAL PRESENTATION
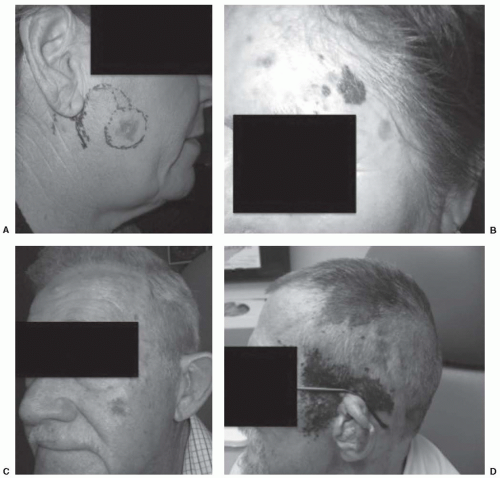
The majority of patients with cutaneous melanoma of the head and neck present in an early stage of disease, as it is uncommon for nodal metastasis to be present at the time of diagnosis. A pigmented lesion may have been present for many years, but it is not until one has undergone substantial change in its clinical appearance that prompts an evaluation with a biopsy. The classic mnemonic of “ABCDE” of pigmented lesions represents an important reminder in public awareness of the warning signs of melanomas, as the vast majority of melanomas (>70%) arise in a preexisting mole. These signs include Asymmetry, Border irregularity, Color variegation, Diameter >6 mm, and Evolution. These lesions may also present as areas that bleed after minor trauma, such as hair brushing or shaving, and patients may complain of itching at the site. Other clinical features associated with cutaneous melanomas include ulceration, regression, and nonpigmented lesions. It is important that the clinician evaluate the surrounding skin for the presence of satellitosis, which represents stage IIIB or IIIC disease, even when nodal metastases are absent (Fig. 24-2).
Nodal metastasis is often subclinical in early-staged patients yet is present in 20% to 30% of patients with T2 lesions, and the incidence of occult nodal metastasis increases substantially in thicker tumors. One of the more challenging areas of the management of melanoma of head and neck involves patients with a regionally metastatic melanoma with an unknown primary tumor. It is important that the treating team perform a careful and detailed clinical history to elicit a history of a regressed lesion or a previously biopsied “benign” nevus. DMs have a propensity for neurotropism, and eliciting signs and symptoms of this aggressive subtype is important in the evaluation of patients with head and neck melanoma.
Diagnostic Staging and Evaluation
The evaluation of a suspected head and neck melanoma entails surgical biopsy, which may be performed as either an excisional biopsy or incisional biopsy, depending on the anatomical location and size of the lesion. Ideally, an excisional biopsy with 1 to 2 mm margins is preferred, which will allow adequate pathological analysis of the entire specimen for staging, without disrupting the lymphatics should an SLNB be necessary. It must be stated that an excisional biopsy does not suffice for surgical management of a melanoma; appropriate surgical margins should be taken at a separate procedure. An incisional or punch biopsy may be performed for large lesions and for those in cosmetically critical areas, such as the nose, eyelid, or ear. In these situations, a complete excision may require significant reconstruction and rotational flaps, which is best performed after definitive resection has been completed. The general principles for the biopsy for a suspected melanoma include representative lesion sampling, adequate depth, and proper specimen orientation. Shave biopsies are often performed for cutaneous lesions, but may not provide adequate representation of the depth of the lesion when performed for a pigmented lesion. This is primarily due to transection of the base of the melanoma, which will impact appropriate tumor staging of the patient. It is also difficult for pathologists to provide a complete histopathological staging of a shave biopsy and thus an incisional biopsy or punch biopsy may be necessary for suspicious pigmented lesion of the head and neck that cannot be assessed with an excisional biopsy.
FIGURE 24-2. Pigmented lesions of the head and neck. A: Melanoma in situ.B: Thin melanoma of the forehead. C: Thick melanoma of the midface. D: Satellitosis.
The appropriate histopathological staging criteria of a biopsied pigmented lesion are outlined in Table 24.2. The pathological reporting of these discrete criteria provides the treatment in the appropriate staging criteria and determines the need for any further evaluation and/or any diagnostic workup or treatment. Use of a pathology template for melanoma has been shown to improve proper staging of patients, particularly when performed as part of an established multidisciplinary group.56
Updates to AJCC Staging. The staging evaluation for melanoma of the head and neck are based on the seventh edition of the TNM staging system of the American Joint Committee on Cancer (AJCC), which was published in 2009 and is provided in Tables 24.3 and 24.4.12 Thin melanomas are defined as ≤1 mm in thickness, intermediate are 1.01 to 4 mm in thickness, and thick melanomas are >4 mm. Stage III patients are defined as those with any nodal metastasis or in-transit metastasis, and stage IV represents distant metastatic disease.
The updated staging system had several differences from previous editions. Substantively, the increasing recognition that mitoses are an adverse prognostic features has been incorporated in the definition of Tlb lesions, which broadens the indications for SLNB in early-staged patients and changes the prognosis for previously staged Tla patients. Clark levels are no longer used in the staging system with some exceptions (i.e., T1 lesions without information about mitotic rate), although pathologists continue to utilize it in pathology reports. Immunohistochemical analysis of sentinel lymph nodes with a melanoma marker (HMB-45, Tyrosinase, MART1, MelanA) is now considered standard of care in pathologically negative nodes, and immunohistochemically positive nodes are categorized as micrometastatic disease. The staging system also added serum lactate dehydrogenase (LDH) levels to the evaluation of patients with stage IV disease.
TABLE 24.2 Key Histopathological Features of Melanoma Primary Tumors
TABLE 24.3 2009 AJCC TNM Staging Categories for Cutaneous Melanomas
T Classification
Thickness (mm)
Ulceration/Mitoses
Tis
NA
NA
T1
≤1.00 mm
a: Without ulceration and mitoses < 1/mm2
b: With ulceration or mitoses > 1/mm2
T2
1.01-2.00
a: Without ulceration
b: With ulceration
T3
2.01-4.00
a: Without ulceration
b: With ulceration
T4
a: Without ulceration
b: With ulceration
N Classification
No. of Metastatic Nodes
Nodal Burden
NO
0
N/A
N1
1
a: Micrometastasis
b: Macrometastasis
N2
2-3
a: Micrometastasis
b: Macrometastasis
c: In-transit metastases/satellites without metastatic lymph nodes
N3
4+ nodes, or matted nodes, or intransit metastases/satellites with metastatic lymph nodes
M Classification
Site
Serum LDH
MO
No distant metastases
N/A
M1a
Distant skin, subcutaneous, nodes
Normal
M1b
Lung
Normal
M1c
All other visceral metastases Any distant metastasis
Normal Elevated
N/A, not applicable; LDH, lactate dehydrogenase. Micrometastases are diagnosed after sentinel lymph node biopsy; macrometastases are defined as clinically detectable nodal metastases confirmed pathologically.
Source: From Balch CM, Gershenwald JE, Soong SJ, et al. Final version of the 2009 AJCC melanoma staging and classification. JCO. 2009;27:6199-6206. Reprinted with permission from the American Society of Clinical Oncology.
Evaluation of Stages 0 to II Melanoma. The diagnostic evaluation of melanomas of the head and neck outlined in Figure 24-3 is based on the current National Comprehensive Cancer Network (NCCN) guidelines.57 In patients with stages 0 to II melanoma, histological analysis of the primary tumor is the major diagnostic study, and for patients with thin melanomas without highrisk features, a thorough history and physical examination may suffice. For patients with ulcerated lesions, imaging of the head and neck may be beneficial, as this subset of patients are at a higher risk of harboring lymph node metastasis. This may be either with computed tomography (CT) of the head and neck or with an ultrasound (US) of the head and neck. The advantage of the US is the potential opportunity to perform a fine-needle aspiration of a suspicious lymph node, but it does not provide the same anatomic detail that actual imaging of the head and neck provides. However, staging can be personalized based on patient factors and physician preference. At our institution, the majority of patients with intermediate-thickness or thick melanomas will undergo imaging of the regional lymphatic basins with either a US or a CT, particularly if ulceration is present. Routine chest x-rays may optionally be performed for patients with IIB to IIC disease to evaluate for lung metastases. Chest x-ray, CT scans, or other imaging should also be performed if signs or symptoms are present that suggest the presence of distant metastases (i.e., pain, dyspnea, neurologic symptoms). Surgical staging of the lymph nodes will be discussed in forthcoming sections.
Clinical staging includes microscopic evaluation of the primary tumor, and clinical and radiologic evaluation for metastases. Pathologic staging includes microscopic evaluation of the primary tumor, and microscopic evaluation of the regional lymph nodes after partial (SLNB) or complete lymphadenectomy. Pathologic stage 0 and stage IA do not require microscopic evaluation of regional lymph nodes for classification.
Source: From Edge SB, Byrd DR, Compton, CC, et al. AJCC Cancer Staging Manual. 7th ed. New York, NY: springer-Veralg; 2010:326, with permission.
Evaluation of Stages III to IV. Patients who are identified as harboring nodal metastasis, whether occult or clinical, should undergo baseline staging studies to exclude the presence of distant metastasis. These may include CT of the chest, abdomen, and pelvis; an MRI of the brain; and determination of serum LDH. More recently, the role of PET-CT for the evaluation of stage III melanoma has been explored and does provide effective baseline staging in this group of patients. The caveat to the use of PET for staging is the resolution for the detection of small metastases, as lesions smaller than 1 cm may be better appreciated on axial imaging. In similar manner, patients with in-transit metastasis require a formal metastatic workup. The timing of these studies should be at the discretion of the multidisciplinary team, but is often performed after local-regional treatment has been completed. Due to emerging therapeutic options, molecular testing for activating mutations in the BRAF, NRAS, and KIT genes should be strongly considered in patients with unresectable regional and distant metastases.29
Role of SLNB. As the status of the lymph nodes remains the most powerful prognostic factor for patients with head and neck melanoma, proper staging of the lymphatics is one of the major diagnostic criteria for patients with melanoma of the head and neck.58 Patients who are node negative generally do not require any adjuvant therapy. Conversely, those with nodal metastasis, even when present at microscopic levels, should be considered for adjuvant systemic therapy (discussed separately). Controversy regarding the management of regional lymphatics in melanoma has persisted for decades, and elective nodal dissection was frequently recommended for patients with melanoma in the past. However, as only approximately 20% of patients harbor occult metastasis, a substantial number of patients were subjected to unnecessary nodal dissections, which can result in significant morbidity.59 Alternatively, observation alone is associated with adverse outcomes, compared with elective nodal dissection for certain groups of patients. With the increased recognition that most patients with intermediate-thickness melanomas do not benefit from elective nodal dissection, the staging philosophy for melanoma has changed substantially in the past decade.
Elective regional dissection has been supplanted by SLNB as the standard of care in the initial evaluation of the majority of patients with cutaneous melanoma. SLNB was first proposed as an effective staging tool by Cabanas in 1977 for the management of penile squamous cell carcinomas.60 The technique was subsequently championed by Morton et al. for the diagnostic evaluation of metastatic melanoma, based upon the principle that melanoma metastasizes in an orderly fashion to the firstechelon draining lymphatic basin.61 In the evaluation and staging of patient with melanoma, SLNB offers the following advantages: (a) increased sensitivity to detect regional metastases, (b) limited morbidity compared with elective nodal dissection, (c) identification of patients who may benefit from further therapies such as a neck dissection or systemic adjuvant therapy, and (d) potentially halting the regional progression of disease.
Although initially met with skepticism, SLNB is now the established approach for defining the presence of occult metastasis.62 The rich and complex organization of the lymphatics of the head and neck make localization of the immediately draining nodes potentially more challenging, as compared with other sites. Moreover, initial published reports validating the role of this staging technique focused primarily on truncal and limb melanomas, with few studies having enrolled patients with lesions located in the head and neck.63 One study has suggested that head and neck sites were associated with higher regional failure rates after a negative SLNB.64 More recent studies with long-term followup of patients with head and neck melanoma suggest a regional failure rate of 4% to 8% after a negative SLNB, which is comparable to that for other anatomic sites.65,66,67 Numerous studies have now validated SLNB for cutaneous melanomas of the head and neck, with a negative predictive value close to 98% and a false-negative rate of 5%.68,69
Only gold members can continue reading. Log In or Register to continue