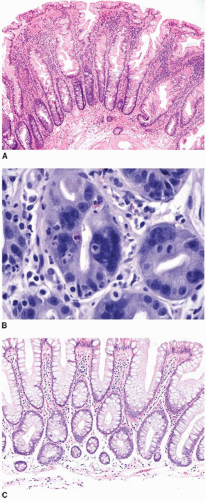
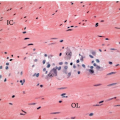
 FIGURE 4.1: Microvesicular hyperplastic polyps are composed of serrated crypts that are narrow at their bases with wide openings at the surface. The crypts contain goblet and nongoblet mucinous cells with abundant cytoplasm and small basally oriented nuclei (A). Cytologic atypia, including multinucleated cells, is occasionally encountered (B). Goblet cell-rich hyperplastic polyps display serration mostly on the surface and are largely composed of goblet cells (C). |
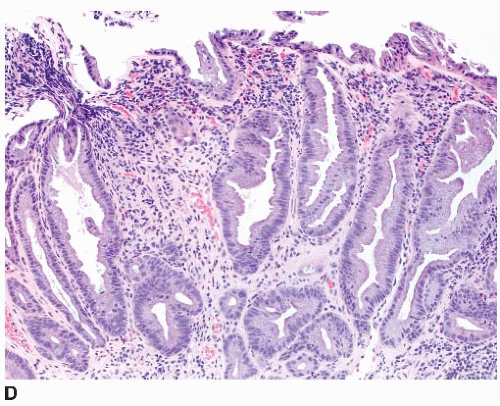 FIGURE 4.1: (Continued) Mucin-poor hyperplastic polyps display a serrated architecture similar to microvesicular hyperplastic polyps, but contain somewhat mucin-depleted epithelial cells and decreased goblet cells (D). |
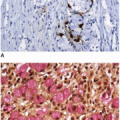
(60% to 70%) show the CIMP.14,22 Loss of MGMT and MLH1 immunoexpression is limited to the superficial epithelial cells, but reflects the nonproliferative nature of the polyp surface, rather than underlying microsatellite instability (MSI). Early investigations reported MGMT and MLH1 promoter methylation in 40% and 72% of sessile serrated polyps, respectively.7,14,17,23 Unfortunately, these studies utilized qualitative, rather than quantitative, assays, and more recent data indicate that sessile serrated polyps are microsatellite stable with preserved MLH1 function.24
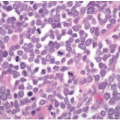
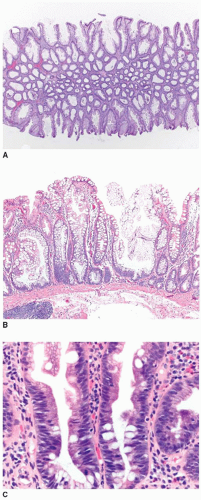 FIGURE 4.2: Sessile serrated polyps are broad-based plaques composed of elongated crypts that show persistent dilatation at their bases (A). They also display architectural abnormalities, including laterally branched, or budding, crypts oriented parallel to the muscularis mucosae (B). Atypical, hyperchromatic nuclei with pseudostratification may extend beyond the crypt bases into the midcrypt region (C). |
Table 4.1 Diagnostic Criteria of Sessile Serrated Polyp | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
development, as discussed in Chapter 3. Patients with a few, small adenomas are at low cancer risk, whereas those with more numerous adenomas, large polyps (>1 cm), or high-grade dysplasia are at a higher risk for cancer development and undergo more rigorous surveillance.
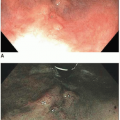
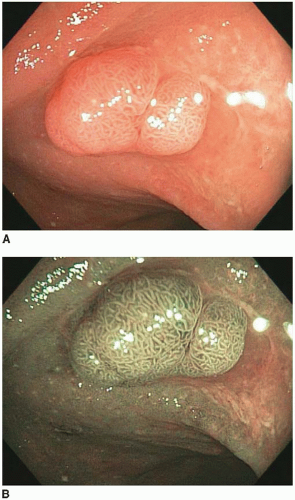 FIGURE 4.3: A sessile tubular adenoma of the right colon is slightly more erythematous than the background mucosa (A). Narrow band imaging accentuates the irregular pit pattern characteristic of dysplastic (adenomatous) polyps (B). |
Related posts:
 Embryology, Anatomy, and Normal Histology of the Colorectum and Appendix
Embryology, Anatomy, and Normal Histology of the Colorectum and Appendix
 Morphologic Classification of Colorectal Epithelial Tumors
Morphologic Classification of Colorectal Epithelial Tumors
 Pathologic Staging Issues: Implementation of the TNM Staging System
Pathologic Staging Issues: Implementation of the TNM Staging System
 Noninvasive Biomarkers and Early Detection of Colorectal Cancer
Noninvasive Biomarkers and Early Detection of Colorectal Cancer
 Emerging Endoscopic Techniques in the Management of IBD-related Neoplasia
Emerging Endoscopic Techniques in the Management of IBD-related Neoplasia
 Nonmucinous Epithelial Tumors of the Appendix
Nonmucinous Epithelial Tumors of the Appendix
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


