Nonmucinous Epithelial Tumors of the Appendix
Rhonda K. Yantiss
The vast majority of clinically important appendices epithelial neoplasms are mucinous tumors, as discussed in Chapter 19, whereas nonmucinous neoplasms are less frequent. These tumors generally simulate their colonic counterparts in that they display tubular, villous, or serrated crypt architecture. Most nonmucinous neoplasms are detected in appendectomy specimens obtained for presumed appendicitis or in appendices removed during procedures performed for other reasons. Invasive nonmucinous adenocarcinomas are even more rare, and their clinicopathologic features and biologic potential are not well described. Most arise in association with precursor lesions, such as goblet cell carcinoid tumors and serrated neoplasms. Their pathologic stage groupings essentially mirror those of colorectal neoplasms.
COLONIC-TYPE ADENOMAS
Clinical Features
Colonic-type adenomas are the least common type of epithelial neoplasm in the appendix. Appendiceal adenomatous polyps are typically asymptomatic. Virtually all of them are identified in prophylactic colectomy specimens from patients with familial polyposis, although rare sporadic lesions are occasionally encountered. Thus, they show an equal predilection for males and females and occur in pediatric patients as well as adults.1 Cancer development occurs in less than 20% of appendiceal adenomas, probably reflecting the relatively small size of these lesions.2,3
Pathologic Features
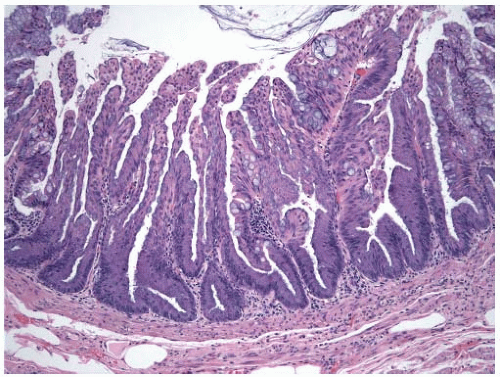
Colonic-type adenomas of the proximal appendix likely represent extension of sessile colonic polyps into the appendiceal orifice. Lesions that develop in the appendix appear as polypoid projections that protrude into the lumen (Figure 20.1). Unlike appendiceal mucinous neoplasms, they do not circumferentially involve the mucosa but are sharply demarcated from adjacent nonneoplastic mucosa. They resemble their colonic counterparts and contain crowded, tubular crypts lined by overtly dysplastic epithelial cells with elongated, hyperchromatic nuclei (Figure 20.2).
SERRATED LESIONS OF THE APPENDIX
Clinical Features
Serrated appendiceal polyps tend to develop in older adults and show an equal sex distribution.4,5 In situ lesions are asymptomatic and incidentally detected in appendices removed for other reasons, including colon cancers, and thus, early evidence pointed toward a strong relationship between serrated appendiceal lesions and colon cancer. Indeed, retrospective data suggested that nearly 50% of serrated appendiceal neoplasms occurred in patients with proximal colonic carcinomas.6 However, recent reports have shown that serrated appendiceal neoplasms are more commonly observed in resection specimens obtained for medical reasons, such as appendicitis, enterocolitis, or indications unrelated to the gastrointestinal tract.4,5
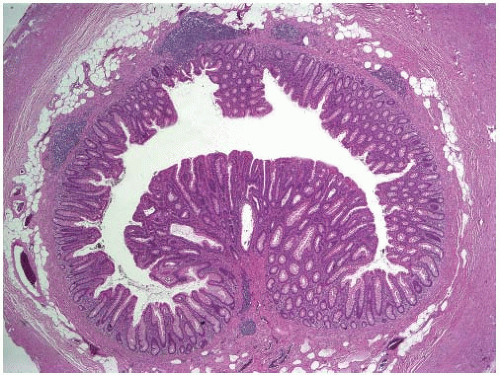 FIGURE 20.1: A sporadic colonic-type adenoma in the appendix has a polypoid appearance and is sharply demarcated from the adjacent nonneoplastic epithelium. (Photograph Courtesy of Dr. Henry Appelman, University of Michigan, Ann Arbor, MI.) |
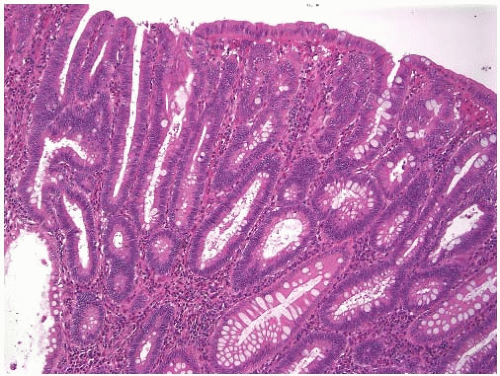 FIGURE 20.2: A sporadic colonic-type adenoma of the appendix contains crypts lined by neoplastic cells with elongated, hyperchromatic nuclei similar to its counterpart in the colorectum. (Photograph Courtesy of Dr. Henry Appelman, University of Michigan, Ann Arbor, MI.) |
Pathologic Features
Serrated appendiceal neoplasms show a spectrum of morphologic features similar to serrated colorectal polyps. Most lack dysplasia and resemble colonic hyperplastic polyps or sessile serrated polyps. Hyperplastic polyps typically protrude into the lumen and appear as plaque-like excrescences but do not involve the entire luminal circumference (Figure 20.3). They contain serrated crypts and mucinous epithelial cells similar to “microvesicular” hyperplastic polyps of the colorectum (Figure 20.4). Sessile serrated polyps circumferentially involve the appendiceal mucosa (Figure 20.5). These lesions contain elongated, somewhat dilated, serrated crypts with lateral branching, dystrophic goblet cells, and mild cytologic atypia (Figure 20.6).
Dysplastic serrated polyps of the appendix are classified as either serrated adenomas or sessile serrated polyps with dysplasia. Serrated adenomas contain serrated crypts lined by cells with abundant eosinophilic cytoplasm and pencillate nuclei (Figure 20.7). Sessile serrated polyps with dysplasia may harbor nondysplastic areas that resemble hyperplastic polyp or sessile serrated polyp intimately admixed with overtly dysplastic crypts that display a tubular, villous, or serrated appearance. Less frequently, sessile serrated polyps with dysplasia contain dilated, laterally branched crypts lined by dysplastic epithelium (Figure 20.8).
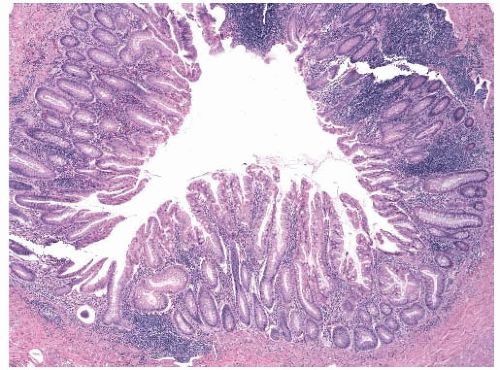 FIGURE 20.3: A hyperplastic polyp protrudes into the lumen of the appendix. |
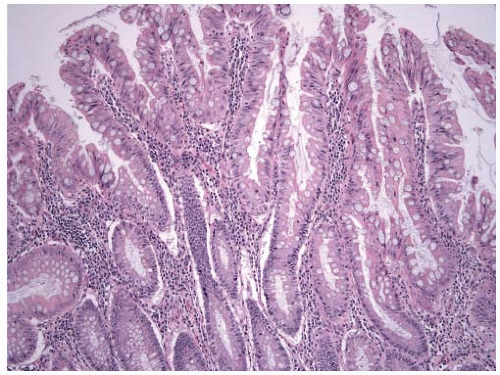 FIGURE 20.4: Hyperplastic appendiceal polyps contain serrated crypts lined by goblet and nongoblet mucinous epithelial cells, similar to colonic microvesicular polyps. |
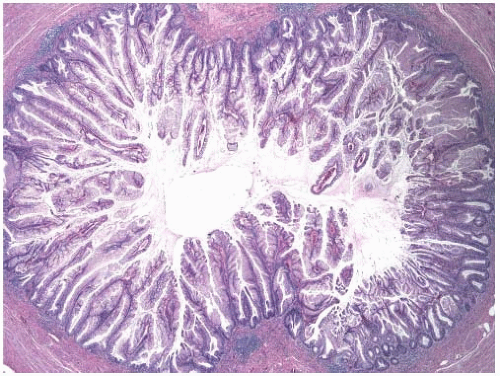 FIGURE 20.5: Sessile serrated polyps circumferentially involve the mucosa of the appendix. Dilated, elongated crypts expand the mucosa. |
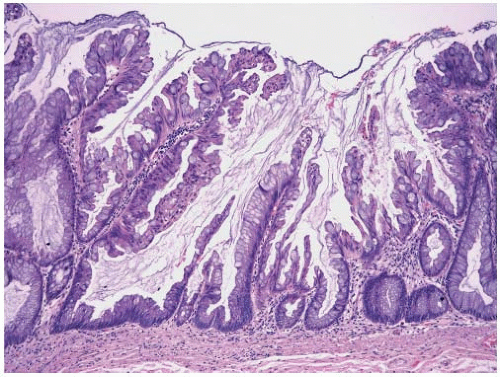 FIGURE 20.6: This sessile serrated polyp of the appendix contains distended crypts, some of which show branching above the muscularis mucosae. |
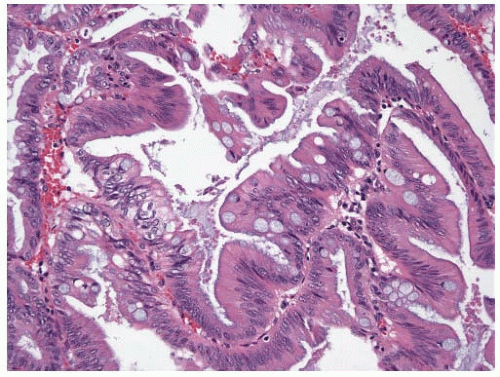 FIGURE 20.7: Serrated adenomas of the appendix contain serrated crypts lined by cells with abundant eosinophilic cytoplasm and pencillate nuclei. |