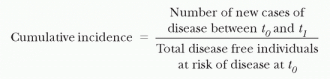
Although this measure describes the total proportion of new episodes occurring in a time period, it does not describe when in the time period they occurred. For the cumulative incidence of HAIs, the period implied is the beginning of hospitalization until a first event or until discharge. However, patients do not stay in the hospital and remain at risk for exactly the same period of time. Thus, comparing the cumulative incidence of HAI among patient groups with differing lengths of stay may be very misleading.
determine if they differ with regard to their presence of risk factors of interest.
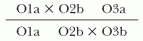
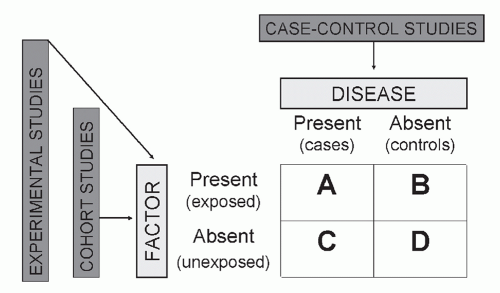 Figure 9.1. Study designs. (Adapted from Lautenbach E. Epidemiological methods in infection control. In: Lautenbach E, Woeltje K, eds. Practical Handbook for Healthcare Epidemiologists. Thorofare, NJ: Slack; 2004:65.) |
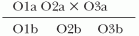
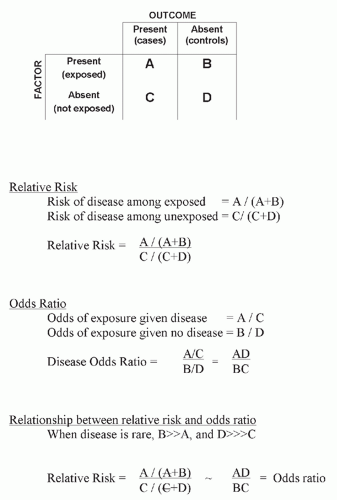 Figure 9.2. Relative risk and odds ratio. (Adapted from Lautenbach E. Epidemiological methods in infection control. In: Lautenbach E, Woeltje K, eds. Practical Handbook for Healthcare Epidemiologists. Thorofare, NJ: Slack; 2004:65.) |
bias (i.e., distortion in the estimate of effect resulting from the manner in which the subjects are selected for the study). For example, a common type of information bias in case-control studies is recall bias. One may compare the patients with an FQREC HAI to a random sample of noninfected controls in an effort to identify the risk factors for FQREC HAI. If the patients with an FQREC HAI are aware of their diagnosis, they may be more likely to try to identify the possible reasons for experiencing a resistant infection. If this group is more likely to remember recent antibiotic use than are controls, the association between recent antibiotic use and FQREC HAI will be spuriously strengthened.
TABLE 9.1 Hierarchy of Quasi-Experimental Study Designs | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||


Related posts:
 Occupational Health Services
Occupational Health Services
 The Practice of Epidemiology in Community Hospitals
The Practice of Epidemiology in Community Hospitals
 Epidemiology and Control of Healthcare-Acquired Infections in Limited-Resource Settings
Epidemiology and Control of Healthcare-Acquired Infections in Limited-Resource Settings
 The Intensive Care Unit, Part A: HAI Epidemiology, Risk Factors, Surveillance, Engineering and Administrative Infection Control Practices, and Impact
The Intensive Care Unit, Part A: HAI Epidemiology, Risk Factors, Surveillance, Engineering and Administrative Infection Control Practices, and Impact
 Urinary Tract Infections
Urinary Tract Infections
 Infections of Burn Wounds
Infections of Burn Wounds
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


