Chapter 57 Endometrial Cancer
Endometrial carcinoma is the most frequent gynecologic malignancy diagnosed in the United States and European countries, and it is the fourth most common cancer in women. Because most patients present with early-stage disease, their prognosis is usually favorable. The relative 5-year survival rate is 84% for all patients. Patients with disease confined to the uterus have a 5-year relative survival rate of 96%, compared with 67% for those with regional involvement.1
Epidemiology and Etiology
Epidemiology
The incidence of endometrial cancer in the United States is 23.5 cases per 100,000 women, and it has remained more or less stable since 1995.1 The U.S. incidence is among the highest in the world. European countries report incidence rates ranging from 15 to 20 cases per 100,000 women.2 The American Cancer Society estimates that a total of 43,470 new cancers of the uterus will be diagnosed in 2010.1 This represents 5.8% of the estimated 739,940 new female malignancies, and it is the most common gynecologic malignancy and the fourth most common cancer in women. The mortality rate for uterine cancer in the United States is 4.1 deaths per 100,000, and the estimate for 2010 is 7,950 deaths, which is 2.5% of all cancer deaths among women and 25% of all deaths from gynecologic malignancies. The mortality rate decreased from 5.3 to 4.1 deaths per 100,000 women between 1973 and 1995 and has remained stable since 1995. On January 1, 2007, in the United States there were approximately 575,108 women alive who had a history of cancer of the corpus uteri.
Uterine cancer is typically a cancer of postmenopausal women between 55 and 85 years old, with incidence rates exceeding 80 per 100,000 women aged 60 to 85 and a peak incidence of 90 per 100,000 women aged 65 to 69.1 Less than 5% of the patients are younger than age 40 years. Uterine sarcomas also manifest primarily in the postmenopausal population. Leiomyosarcomas occur at an earlier age than carcinosarcomas.3
Etiology
The cause of endometrial carcinoma is related to exposure of the endometrium to unopposed estrogens. Many studies have documented the association of endometrial cancer with increased exogenous or endogenous estrogen exposure.4 Early menarche, late menopause, obesity, nulliparity, infertility, and estrogen-producing ovarian tumors are classically associated with the development of endometrial cancer. In obese women, elevated estrogen levels caused by increased peripheral conversion of androstenedione may be the underlying mechanism for the increased risk. Endometrial cancer has also been associated with conditions such as hypertension and diabetes, but it is not clear whether these are true independent risk factors or related to obesity.5 Unopposed exogenous estrogen levels have strong association with the risk of endometrial cancer.6 The use of tamoxifen for the prevention or treatment of breast cancer has been documented to statistically increase the risk of subsequent endometrial cancer.7–10 Despite its antiestrogen effects on breast tissue, tamoxifen has some weak estrogenic effects on other organs of the body, including the uterus, which accounts for this risk.
Patients who have endometrial biopsies confirming complex hyperplasia with atypia have a 30% to 40% risk of subsequent development of endometrial cancer. Hyperplasia with atypia is considered a premalignant phase of endometrioid carcinoma and has a similar origin.11
An increased risk associated with a family history of endometrial cancer has been observed, especially in women younger than 50 years, but less than 1% of all endometrial cancers were attributable to familial and potentially genetic factors.12–14 Familial clustering of ovarian and endometrial cancers specific to the endometrioid morphology has been reported.15,16 The risk of developing other malignancies, especially of the colon and breast, is increased after the diagnosis of endometrial carcinoma.15,16 Women with mutations in the MLH1, MSH2, or MSH6 genes, which are responsible for the hereditary nonpolyposis colorectal cancer (HNPCC) syndrome, are at increased risk for developing endometrial cancer.17–19 HNPCC, or Lynch syndrome, is classified based on the presence or absence of tumors other than colorectal cancers. HNPCC syndrome type II patients have a high risk of endometrial cancer, second only to that of colorectal cancers.20,21 These women have a 20% risk of developing endometrial cancer before 50 years of age, which increases to 60% by age 60 years.
Prevention and Early Detection
No measures that may contribute to prevention of endometrial cancer other than avoiding unopposed estrogen use and avoiding obesity have been identified. Prophylactic hysterectomy is recommended in patients with known hyperplasia with atypia,11,22,23 and prophylactic hysterectomy and oophorectomy is advised in HNPCC type II gene carriers, for whom the risk of concurrent or subsequent endometrial cancer is substantial.20,21,24
Screening for endometrial cancer has not been performed in the general population. The early symptoms and favorable prognosis of this disease preclude efficacy of population screening.25 Vaginal ultrasound studies alone have not been found effective for screening purposes.26 Prompt analysis of every patient with postmenopausal or abnormal vaginal bleeding with vaginal ultrasound studies and endometrial biopsy is indicated.
Screening of patients using tamoxifen has been suggested. However, the characteristic hyperplastic aspect of the endometrium at ultrasound studies leads to high false-positive rates and frequent invasive diagnostic procedures in asymptomatic tamoxifen users.27,28 In a prospective ultrasound screening study of 247 tamoxifen users,27 it was shown that, of 52 asymptomatic patients with a thickened endometrium, most had an atrophic endometrium and only 1 had cancer, whereas in 2 of 20 patients with vaginal bleeding, endometrial cancer was diagnosed. The study authors concluded that routine ultrasound screening is not indicated in asymptomatic women using tamoxifen but that all women with abnormal bleeding should be evaluated.
Screening programs of gene carriers for the HNPCC syndrome not electing prophylactic surgery have shown increased efficacy when using annual endometrial biopsy in addition to vaginal ultrasonography. An evaluation of gynecologic surveillance among 175 mutation carriers (503 surveillance visits during 759 person-years at risk) using vaginal ultrasonography and endometrial biopsy at 94% and 74%, respectively, of the visits showed that 11 of 14 endometrial cancer cases were diagnosed by surveillance and 8 by endometrial biopsies. Vaginal ultrasonography indicated only four patients with endometrial cancer and missed 6 other cases. Endometrial biopsy detected 14 additional cases of potentially premalignant hyperplasia. The stage distribution and survival tended to be more favorable, although not statistically so, in the 14 cases of endometrial cancer in the surveillance group (no deaths) than in a group of 83 symptomatic mutation carriers of whom 6 died of endometrial cancer.29
Pathology and Pathways Of Spread
Pathology
Almost all uterine epithelial cancers are adenocarcinomas. The World Health Organization (WHO) has described several subtypes (Table 57-1). The most common type of endometrial adenocarcinoma is the endometrioid type, which accounts for 75% of cases.30,31 Other histologic types, also referred to as nonendometrioid endometrial carcinomas, include serous (5% to 10%), mucinous (1% to 3%), and clear cell (1% to 5%) carcinomas. Uterine mesenchymal and mixed tumors, usually called the uterine sarcomas, include leiomyosarcoma, endometrial stromal sarcoma, and carcinosarcoma (or malignant mixed müllerian tumor). The WHO classification of mesenchymal and mixed tumors of the uterus is summarized in Table 57-2. Carcinosarcoma is the most common type of uterine mesenchymal and mixed tumor (45%), followed by leiomyosarcoma (40%) and endometrial stromal sarcoma (10% to 15%). Carcinosarcomas are composed of malignant epithelial and stromal components; and because of this biphasic appearance, their origin has long been debated. Based on molecular genetic analysis, the current opinion is that these cancers should be considered metaplastic carcinomas. Clinical data support this view that carcinosarcomas should be considered high-risk carcinomas, particularly because the epithelial component is usually of high grade.31–33
TABLE 57-1 World Health Organization Histologic Classification of Epithelial Tumors of the Uterus
TABLE 57-2 World Health Organization Histologic Classification of Mesenchymal and Mixed Tumors of the Uterus
| Mesenchymal Tumors |
| Mixed Epithelial and Mesenchymal Tumors |
Nonendometrioid histologic types have a poorer prognosis. Serous and clear cell carcinomas are uniformly identified in this category. Serous adenocarcinoma was previously called uterine papillary serous carcinoma. It is histologically similar to its ovarian counterpart. Uterine papillary serous carcinoma was first described in 1982 and was found to have a higher rate of failure within the abdomen, as in ovarian cancer.34,35 This entity can be confused with the papillary villoglandular subtype of endometrioid adenocarcinoma, which carries a significantly more favorable prognosis. Serous carcinoma is frequently diagnosed at a higher stage than endometrioid adenocarcinomas. Clear cell carcinoma has been reported to have the same poor prognosis, with more advanced disease at diagnosis.36,37 Serous and clear cell carcinomas have been shown to have outcomes similar to grade 3 endometrioid carcinoma.38,39
Adenosquamous cell carcinoma has been suggested by some investigators to be another poor histologic subtype,36,37 but others think the prognosis of these patients is no different from that for the typical endometrioid adenocarcinoma.40,41 Zaino and colleagues41 evaluated a large population of patients who were part of a Gynecologic Oncology Group (GOG) study and found a parallel between the glandular grade and the degree of differentiation in the squamous component. It was subsequently suggested that the name of this histologic subtype should reflect the lack of importance of this feature by calling it adenocarcinoma with squamous differentiation.
Endometrial hyperplasia frequently precedes endometrial carcinoma. Endometrial hyperplasia is considered a precursor of endometrioid carcinoma, and endometrial intraepithelial carcinoma has been associated with the development of nonendometrioid carcinoma. The International Society of Gynecological Pathologists has identified two architectural forms of endometrial hyperplasia, simple and complex. Endometrial hyperplasia displaying marked architectural abnormalities is designated complex hyperplasia, whereas lesions with a lesser degree of architectural abnormalities are designated simple hyperplasia. Atypical nuclear changes can be associated with the simple or complex types and are regarded separately from hyperplasia that is not displaying atypia. Progression of simple hyperplasia to endometrioid carcinoma is rare (<2%), whereas progression to carcinoma occurs in 30% to 40% of the patients with simple and complex hyperplasia with atypia.11,22,23,42,43 The risk of subsequent endometrial cancer warrants hysterectomy in patients with hyperplasia displaying atypia.
Not all endometrial cancers arise in a setting of atypical hyperplasia. Nonendometrioid cancers, especially serous carcinomas, are related to endometrial intraepithelial carcinoma, which appears to represent malignant transformation of atrophic endometrium. It is found in the adjacent endometrium of up to 90% of serous carcinomas.44
Pathways of Spread
Most endometrial cancers remain confined to the uterine body for a long time. The initial spread occurs by local extension along the endometrial surface. Subsequent growth continues in the radial and longitudinal directions. Longitudinal growth may result in involvement of the lower uterine segment and the cervix, initially involving the endocervical glands and later spreading by cervical stromal invasion. The tumor can also extend along the cornua to the fallopian tubes. Radial growth results in myometrial invasion, initially superficially and later penetrating to the subserosa and the serosa. Two patterns of myometrial invasion have been described: an expansive growth pattern with pushing borders and an infiltrating growth pattern with cancer cells and nests penetrating the myometrium haphazardly.45,46 The infiltrating growth pattern is associated with frequent lymphovascular space invasion (LVSI) and early lymphatic spread. After the tumor breaches the serosa, transperitoneal dissemination can occur, with a pattern resembling that of ovarian cancer. Occasionally, after extensive penetration of the myometrium or the cervix, direct invasion of the bladder or the rectum may occur, or the tumor may involve the pelvic soft tissues and continue to reach the pelvic sidewall. Peritoneal seeding can result from growth through the serosa or from transtubal spillage of tumor cells into the peritoneal cavity.
As the tumor invades the myometrium more extensively, the risk of lymph node metastasis is higher.47,48 The endometrium has few lymphatics, but after the tumor penetrates the myometrium and especially when it reaches the lymphatic-rich subserosa, spread by lymphatic invasion is common. Lymphatics from the uterine fundus can drain directly to the para-aortic lymph nodes. Typically, the internal and external iliac lymph node groups are the first echelon of spread although isolated para aortic nodal involvement also occurs. Sentinel node detection studies49–51 have shown the sentinel nodes to be located in the obturator, external iliac, and para-aortic regions. Lymphatic spread is also believed to be responsible for involvement of the vagina and for isolated adnexal involvement.
Overall, about 11% of patients with clinical stage I and occult stage II endometrial carcinoma and 5% to 7% of patients with tumors confined to the uterus have pelvic or para-aortic lymph node involvement.47,52 The extent of myometrial penetration correlates strongly with the histologic grade of the tumor, and the depth of invasion and tumor grade correlate with the risk of lymphatic involvement. The risk of intra-abdominal dissemination is higher in patients with nonendometrioid carcinoma. Abdominal involvement of endometrioid carcinoma is associated with other risk factors, such as lymph node involvement, adnexal involvement, and LVSI.
Biologic Characteristics and Prognostic Factors
Biologic Features
Two different types of endometrial carcinoma have been described.53 Type I tumors are estrogen related, are often preceded by hyperplasia, and are typically low-grade endometrioid carcinomas. They usually develop in an estrogen-rich environment (e.g., obesity, premenopausal and perimenopausal phases), and they have a good prognosis. Type II tumors are unrelated to estrogen and develop in atrophic endometrium, presumably preceded by endometrial intraepithelial carcinoma, and they are more often serous and clear cell carcinomas. Patients with type II tumors are older postmenopausal patients; have high-grade, deeply invasive tumors; and have an unfavorable prognosis.31,53 A summary of the differences between these two groups is shown in Table 57-3. The genetic abnormalities involved in the carcinogenesis of endometrial cancer are different for type I and II carcinomas.
TABLE 57-3 Predominant Features of Type I and II Endometrial Cancer
| Characteristic | Type I | Type II |
|---|---|---|
| Clinicopathologic Features | ||
| Estrogen relation | Yes | No |
| Precursor lesion | Hyperplasia | Intraepithelial carcinoma |
| Age | Younger | Older |
| Histologic type | Endometrioid | Nonendometrioid |
| Grade | 1 or 2 | 3 |
| Stage | 1 | More advanced |
| Prognosis | Good | Poor |
| Genetic Features | ||
| Ploidy | Diploid | Aneuploid |
| TP53 mutation | 10-20% (late event) | 60-90% (early event) |
| PTEN inactivation | 35-50% | 5-10% |
| ERBB2 protein overexpression | 10-15% | 20-25% (serous: 60%) |
| EGFR overexpression | 10-30% | 60-80% |
| KRAS mutation | 15-30% | 0-5% |
| Microsatellite instability | 20-30% | 0-5% |
Specific molecular alterations have been found in type I and II endometrial cancers. In type II cancers, TP53 mutations have been found in up to 90% of cases (invasive and intraepithelial carcinomas), suggesting it to be an early event in carcinogenesis. ERBB2 protein overexpression has been reported in a significant proportion (up to 80%) of serous carcinomas. About 20% to 30% of serous carcinomas are found to have amplification of the ERBB2 gene. The ERBB2 gene product, similar to the epidermal growth factor receptor, is a transmembrane receptor protein that plays an important role in the ERBB signaling network that is responsible for regulating cell growth and differentiation. ERBB2 overexpression is associated with aggressive biologic behavior and poor survival. Targeted therapy using trastuzumab (Herceptin), a monoclonal antibody to ERBB2, is a potentially attractive treatment strategy.54,55 However, the one prospective clinical trial testing single-agent trastuzumab in endometrial carcinomas with ERBB2 overexpression or amplification reported no major responses.56 Epidermal growth factor receptor (EGFR) overexpression occurs in 60% to 80% of type II cancers, and it correlates with advanced-stage disease and poor prognosis.57 Targeted therapy with anti-EGFR agents including tyrosine kinase inhibitors such as gefitinib, lapatinib, and erlotinib as well as monoclonal antibodies such as cetuximab is being investigated.58,59 Results thus far have been modest. The National Cancer Institute of Canada (NCI Canada) reported a 12.5% response rate to single-agent erlotinib for chemotherapy-naive tumors. There was no correlation found between response and EGFR gene mutations or amplification.58
No specific abnormalities have been associated with type I cancers in general, which suggests that type I is a heterogeneous group of tumors with different combinations of abnormalities. TP53 mutations have been found in 10% to 20% of type I cancers, are associated with grade 3 tumors, and may be related to dedifferentiation. Mutant TP53 protein expression has been associated with advanced stage and other adverse factors, such as poor differentiation, deep invasion, and poor survival.60,61 More general markers of genetic damage such as DNA aneuploidy have consistently been associated with an inferior outcome.60,62–65
PTEN is frequently altered in endometrioid endometrial carcinomas (37% to 61%) and is considered an early event in carcinogenesis. The loss of PTEN, with consequent activation of the PI3K (phosphatidylinositol-3-kinase)-AKT (serine/threonine-specific protein kinase)-mTOR (mammalian target of rapamycin) signaling pathway, has been found in 32% to 83% of endometrioid-type endometrial carcinomas.66 TOR is the central component of a complex signaling network that regulates cell growth and proliferation and is interconnected with the PI3K/Akt signaling pathway. Studies have shown that PIK3CA mutations are frequently found in association with myometrial invasion, advanced stage, and adverse prognostic factors.60,67,68,69 This suggests a role for mTOR inhibition, and the mTOR pathway is currently regarded an important target for therapy. Phosphorylated mTOR overexpression has been found in both type I and II endometrial carcinomas.70 Phase II trials using mTOR inhibitors including deforolimus, temsirolimus, and everolimus have been performed. The most promising preliminary results thus far have been reported by the NCI Canada in women with chemotherapy-naive disease, in whom a 21% response rate to single-agent therapy with temsirolimus was observed.71 To date no markers of activation of the PI3K/Akt signaling pathway have proven to be predictive of response to mTOR inhibitors in patients.
As listed in Table 57-4, some molecular abnormalities such as PTEN and KRAS mutations, which are considered early events in the development of endometrioid carcinomas, are associated with a favorable prognosis, whereas others predict an unfavorable outcome. In most multivariate analyses, however, the prognostic significance of these molecular markers is lost in the presence of the traditional major prognostic factors: stage, grade, depth of invasion, and histologic subtype. The major promise of the molecular markers is the identification of specific targets for therapy and development of individual, effective therapeutic strategies for patients with advanced and/or metastatic disease.
TABLE 57-4 Prognostic Value of Genetic Abnormalities
| Genetic Abnormality | Prognostic Value |
|---|---|
| Aneuploidy | Decreased survival* |
| TP53 mutation | Decreased survival |
| PTEN inactivation | Conflicting data |
| ERBB2 overexpression | Decreased survival |
| EGFR overexpression | Decreased survival |
| KRAS mutation | Conflicting data |
| Microsatellite instability | No prognostic significance |
* Remains significant prognostic factor in multivariate analysis.
Prognostic Factors
Numerous studies have identified the major prognostic factors in endometrial carcinoma. Comprehensive retrospective analyses and prospective, randomized studies have established the major prognostic factors for survival and relapse to be stage, patient age, histologic cell type, tumor grade, depth of myometrial invasion, and presence of LVSI.48,72,73 Randomized trials have confirmed the prognostic value of these factors.74–76 Among stage I patients, grade has been found to be a major factor, with grade 3 tumors associated with a threefold to fivefold increased risk of relapse and cancer death.77,78 In most studies, grade 2 tumors do not have significantly different outcomes compared with grade 1, and two-tiered grading systems have been proposed to overcome the limited clinical value and poor reproducibility of the intermediate grade.45,79 The binary grading system proposed by Lax and co-workers45 is based on the proportion of solid growth, the pattern of myometrial invasion, and the presence of tumor cell necrosis. In a comparative analysis of the prognostic significance and the interobserver variability of these grading systems in a series of 800 stage I endometrial cancers, the reproducibility of the binary system was not found to be greater than that of the International Federation of Gynecology and Obstetrics (FIGO) grading system, but the prognostic power of the systems was equally strong. A simple two-tiered system, dividing tumors into low or high risk based on the proportion of solid growth (<50% vs. >50%), was shown to have superior prognostic power and greater reproducibility.80 Alternatively, the FIGO grading system may be used as a binary system by dividing tumors into grades 1 and 2 versus grade 3. Such a binary FIGO system has been shown to have strong prognostic significance, and it has the additional advantages of being highly reproducible and familiar to practicing pathologists worldwide.80,81
In most studies, depth of myometrial invasion had less strong prognostic value than tumor grade. Deep invasion, particularly into the outer third of the myometrial wall, has been associated with increased risk of relapse and inferior outcome.72 A diffusely infiltrating pattern of myometrial invasion, as opposed to an expansive growth pattern with pushing borders, has been suggested to be a stronger adverse prognostic factor than the depth of invasion.77,82 Because the effluent lymphatics and capillaries are mainly located in the subserosa, the tumor-free distance from the serosa may prove to be the strongest prognostic factor. In a multivariate analysis of 153 patients, tumor-free distance was found to be a highly significant predictor of relapse and death from disease, stronger than depth of invasion, and to have greater reproducibility.83
LVSI has been found to be a major prognostic factor that significantly and independently increases the risk of relapse, especially distant relapse.76,78,84 In an analysis of 609 patients with stage I to III endometrial cancer, those with LVSI were found to have a 5-year relapse rate of 39%, in contrast to 19% for patients without LVSI (p <.0001). Even in otherwise low-risk stage I disease, the presence of LVSI significantly increased the risk of relapse (28% with vs. 14% without LVSI). In stage I patients with high-risk features, those with LVSI had a 43% relapse rate.84
Clinical Manifestations/Patient Evaluation/Staging
Patient Evaluation
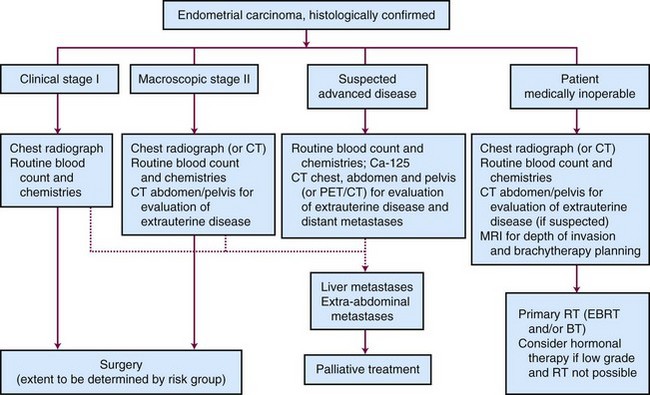
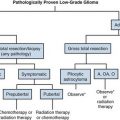
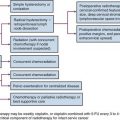
Outpatient procedures, such as transvaginal ultrasonography and endometrial biopsy or aspiration curettage, establish the diagnosis in more than 90% of patients suspected to have endometrial cancer. Various endometrial biopsy tools are available, such as a small Novak curette, Pipelle instrument, or Vabra aspirator, that permit the procedure to be performed without general anesthesia. If these procedures are not conclusive, a formal dilation and fractional curettage (D&C) should be performed, with or without hysteroscopy. Hysteroscopy allows direct visual assessment of the endocervix and the endometrial cavity and can be useful in guiding biopsy of any visible abnormality in symptomatic patients when other procedures have been nondiagnostic. Figure 57-1 presents a diagnostic algorithm for patient workup and evaluation.
Staging
After a diagnosis of malignancy is established, the preoperative evaluation and staging workup are done. Definitive staging according to the FIGO system is based on the surgical and pathology findings. In 2009, a revised FIGO staging system was published, and this has replaced the 1988 FIGO staging system.85 Table 57-5 lists the 2009 FIGO staging and the differences between the 1988 and 2009 systems. (The differences between the 1988 and 2009 systems are seen in a web-only addition to the table, available on the Expert Consult website for this chapter.) The changes in stage IA, IB and IC especially should be kept in mind when evaluating literature data, because FIGO 1988 stage IA and IB have been grouped together in FIGO 2009 as stage IA and because FIGO 1988 stage IC is IB in FIGO 2009. The previous nonsurgical (clinical) FIGO staging system continues to be used for patients not undergoing surgery.
for this chapter.) The changes in stage IA, IB and IC especially should be kept in mind when evaluating literature data, because FIGO 1988 stage IA and IB have been grouped together in FIGO 2009 as stage IA and because FIGO 1988 stage IC is IB in FIGO 2009. The previous nonsurgical (clinical) FIGO staging system continues to be used for patients not undergoing surgery.
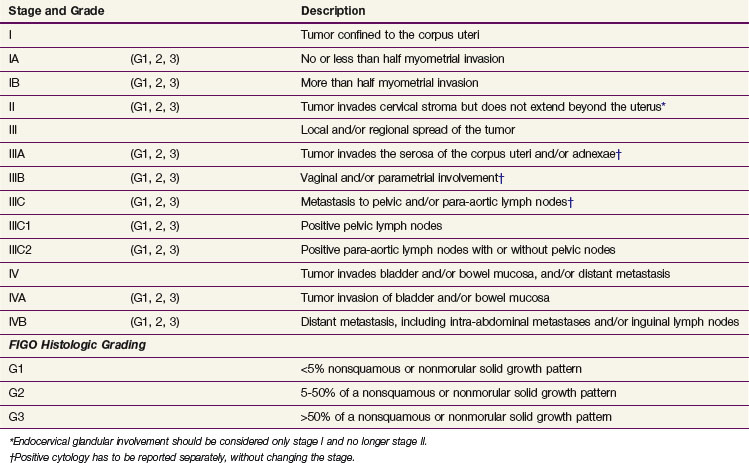
TABLE 57-5 Federation of Gynecology and Obstetrics (FIGO) Surgical Staging System for Endometrial Carcinoma: 2009
| Stage and Grade | Description | |
|---|---|---|
| I | Tumor confined to the corpus uteri | |
| IA | (G1, 2, 3) | No or less than half myometrial invasion |
| IB | (G1, 2, 3) | More than half myometrial invasion |
| II | (G1, 2, 3) | Tumor invades cervical stroma but does not extend beyond the uterus* |
| III | Local and/or regional spread of the tumor | |
| IIIA | (G1, 2, 3) | Tumor invades the serosa of the corpus uteri and/or adnexae† |
| IIIB | (G1, 2, 3) | Vaginal and/or parametrial involvement† |
| IIIC | (G1, 2, 3) | Metastasis to pelvic and/or para-aortic lymph nodes† |
| IIIC1 | (G1, 2, 3) | Positive pelvic lymph nodes |
| IIIC2 | (G1, 2, 3) | Positive para-aortic lymph nodes with or without pelvic nodes |
| IV | Tumor invades bladder and/or bowel mucosa, and/or distant metastasis | |
| IVA | (G1, 2, 3) | Tumor invasion of bladder and/or bowel mucosa |
| IVB | (G1, 2, 3) | Distant metastasis, including intra-abdominal metastases and/or inguinal lymph nodes |
| FIGO Histologic Grading | ||
| G1 | <5% nonsquamous or nonmorular solid growth pattern | |
| G2 | 5-50% of a nonsquamous or nonmorular solid growth pattern | |
| G3 | >50% of a nonsquamous or nonmorular solid growth pattern | |
* Endocervical glandular involvement should be considered only stage I and no longer stage II.
† Positive cytology has to be reported separately, without changing the stage.
TABLE 57-5 Federation of Gynecology and Obstetrics (FIGO) Surgical Staging System for Endometrial Carcinoma: 2009
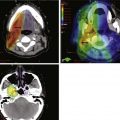
The patient’s general evaluation should include standard blood tests and a chest radiograph. Endometrial carcinoma patients are often elderly and frail and may have a number of concurrent medical problems that influence selection of the appropriate treatment. Computed tomography (CT) and magnetic resonance imaging (MRI) are not routinely performed for patients with clinical stage I disease who will be undergoing surgery, but imaging should be done if locally advanced disease is suspected. The major limitations of CT are its unreliability in assessing myometrial invasion, especially in atrophic uteri, and the failure to detect minimal parametrial, lymph nodal, or local extrauterine invasion.86 The greatest value of CT may be for staging in patients with clinical stage III or IV disease and in medically inoperable patients, for whom CT is useful for evaluating the size and extent of the tumor, for excluding gross extrauterine disease, and for planning of appropriate target volumes for radiation therapy. MRI using an intravenously administered contrast agent is superior to CT in determining myometrial invasion and diagnosing stage II disease.87
Initial studies of the potential role of FDG-PET/CT suggest a promising role for evaluation of relapse during follow-up and for presurgical evaluation of pelvic node metastases. In an analysis of PET/CT in 25 women with suspected relapse during follow-up,88 lesion site–based sensitivity, specificity, positive (PPV) and negative (NPV) predictive values, and accuracy of PET/CT were 94.7%, 99.5%, 94.7%, 99.5%, and 99.0%, respectively. Diagnostic accuracy of PET/CT was evaluated among 37 patients with high-risk endometrial cancer, of whom 9 (24%) had pelvic node metastases on histopathologic analysis. Patient-based sensitivity, specificity, PPV, NPV, and accuracy of PET/CT for detection of nodal disease were 77.8%, 100.0%, 100.0%, 93.1%, and 94.4%, respectively. Nodal lesion site–based sensitivity, specificity, PPV, NPV, and accuracy of FDG-PET/CT were 66.7%, 99.4%, 90.9%, 97.2%, and 96.8%, respectively, showing that PET/CT has a high NPV and may be useful in selecting patients for lymphadenectomy.91
Initial studies of the potential role of FDG-PET/CT suggest a promising role for evaluation of relapse during follow-up and for presurgical evaluation of pelvic node metastases. In an analysis of PET/CT in 25 women with suspected relapse during follow-up,88 lesion site–based sensitivity, specificity, positive (PPV) and negative (NPV) predictive values, and accuracy of PET/CT were 94.7%, 99.5%, 94.7%, 99.5%, and 99.0%, respectively. Other follow-up studies confirmed the efficacy of PET and/or PET/CT in detecting relapse in both asymptomatic and symptomatic patients, with sensitivity of 100% and specificity, PPV, NPV, and accuracy of 83% to 100%.89,90 PET/CT detected relapse in 3 patients with elevated tumor markers but negative CT findings, and altered treatment in 22% of patients.89 Diagnostic accuracy of PET/CT was evaluated among 37 patients with high-risk endometrial cancer, of whom 9 (24%) had pelvic node metastases on histopathologic analysis. Patient-based sensitivity, specificity, PPV, NPV, and accuracy of PET/CT for detection of nodal disease were 77.8%, 100.0%, 100.0%, 93.1%, and 94.4%, respectively. Nodal lesion site–based sensitivity, specificity, PPV, NPV, and accuracy of FDG-PET/CT were 66.7%, 99.4%, 90.9%, 97.2%, and 96.8%, respectively, showing that PET/CT has a high NPV and may be useful in selecting patients for lymphadenectomy.91
Primary Therapy
Surgery
Surgery is the mainstay of the initial treatment of endometrial carcinoma. Surgical evaluation should start with exploration and collection of ascites or peritoneal lavage fluid for cytologic evaluation (although its utility for adding additional prognostic value is questioned). Thorough examination and palpation of the pelvic and abdominal organs and lymph node regions should be performed, and any suspicious sites should be sampled. After initial assessment, the standard surgical procedure is a total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH-BSO). In situations with gross cervical involvement (macroscopic stage II disease), a radical hysterectomy should be considered. Literature data support the use of radical hysterectomy in macroscopic stage II disease to clear potential parametrial disease, although a survival advantage over TAH-BSO and pelvic radiation therapy has not been proved.92,93
The standard surgical approach has traditionally been laparotomy through a midline incision, which allows full exposure of the abdomen, pelvic areas, and lymphatic sites. However, laparoscopic techniques for staging and treatment have been developed, and a number of institutions have evaluated laparoscopic staging and laparoscopic-assisted vaginal hysterectomy, especially for early-stage disease.94–96 The advantages of laparoscopy are the shorter hospitalization and recovery time and decrease of surgical morbidity. Disadvantages are the increased length of the operation and the learning curve involved with laparoscopic techniques. Increased risks of malignant cells in the peritoneal cytology specimen97 and vaginal cuff recurrence or port-site metastases98 have been reported, especially when this technique was first adopted. The importance of early occlusion of the fallopian tubes and uterine artery and avoidance of intrauterine manipulators to prevent such peritoneal spread and vaginal cuff recurrence has been stressed.94,98–100 Retrospective evaluations and initial randomized trials have shown the overall and relapse-free survival rates to be similar to those of laparotomy, with fewer complications and earlier recovery.101,102,103 Other randomized trials are ongoing.104 Laparotomy remains preferable to laparoscopy in very obese patients and in patients with intra-abdominal adhesions.
The role of pelvic and para-aortic lymphadenectomy or lymph node sampling has been widely debated. Determination of nodal involvement has prognostic implications, and in patients with nodal involvement it directs further therapy. The potential therapeutic implications of lymphadenectomy are directly related to the a priori risk of nodal disease in the population studied. Prospective and retrospective studies of lymphadenectomy in patients with clinical stage I or II endometrial carcinoma without extrauterine spread identified at surgery have shown the rates of pelvic and aortic nodal involvement to be 7% to 9% and 2% to 3%, respectively.47,52,105–108 The risk of lymph node involvement varies with the major risk factors, as was demonstrated in the landmark GOG surgical pathologic staging study47 (Table 57-6). Some of these features can be identified at the time of hysterectomy and used to evaluate the indication for lymph node dissection. The addition of lymphadenectomy, especially if pelvic and aortic lymphadenectomies are performed, prolongs operation time and has side effects, such as leg edema (5% to 10%), lymphocysts (symptomatic in 5% to 7%), increased rates of deep vein thrombosis (2%) and small bowel obstruction (up to 5%), and increased blood loss and higher transfusion rates (5% to 10%).85,86,87 Studies suggesting a survival advantage were small, single-center retrospective analyses that were flawed by patient selection and stage migration.107–109 The larger National Cancer Institute and Duke University analyses reported a survival benefit with multiple-site lymphadenectomy for grade 3 cancers, whereas no benefit was found for grade 1 or 2 disease.105,106 Analysis of data from the SEER program did not show benefit from lymphadenectomy for patients with stage I grade 1 or 2 disease but suggested improved disease-specific survival (DSS) for those with stage I grade 3 or more advanced-stage disease.110 Lymphadenectomy should therefore be considered for patients with grade 3 disease, cervical involvement, and high-risk histologic findings.105,106,110,111 It has been shown that if pelvic lymphadenectomy is performed a minimum of 11 nodes should be removed from multiple sites.109 Retrospective analyses are, however, flawed by elimination of patients from earlier-stage categories (i.e., stage migration) and by exclusion of patients at increased surgical risk due to advanced age or concurrent morbidities (i.e., selection bias). For the majority of patients with clinical stage I or occult stage II disease, the risk of nodal involvement is extremely low; therefore it is difficult to justify staging in all patients.112
TABLE 57-6 Risk Factors for Lymph Node Metastases
| Risk Level | Lymph Node Metastasis | |
|---|---|---|
| Pelvic Nodes (%) | Aortic Nodes (%) | |
| All Clinical Stage I | ||
| Low risk | ||
| Grade 1, endometrium only, no intraperitoneal disease | 0 | 0 |
| Moderate risk | ||
| No intraperitoneal disease | ||
| Inner-middle invasion or grade 2 or 3 | 3 | 2 |
| Both factors | 6 | 2 |
| High risk | ||
| Deep invasion | 18 | 15 |
| Intraperitoneal disease | 33 | 8 |
| No Gross Extrauterine Disease | ||
| Low risk | ||
| No invasion or grade 1 with invasion* | <5 | <2 |
| Moderate risk | ||
| All other | 5-10 | <5 |
| High risk | ||
| Grade 3, outer 33% invasion | >10 | >10 |
*Excluding serous or clear cell histology.
Data from Creasman WT, Morrow CP, Bundy BN, et al: Surgical pathologic spread patterns of endometrial cancer. A Gynecologic Oncology Group Study. Cancer 60:2035-2041, 1987.
Two randomized trials investigating the role of lymphadenectomy in clinical stage I endometrial cancer have recently been published. In the U.K. Medical Research Council ASTEC trial 1408 patients were randomized, 704 to TAH-BSO with lymphadenectomy and 704 to TAH-BSO alone.113 The baseline characteristics were well balanced between the groups: 9% had any nodal involvement. The results showed no benefit of lymphadenectomy: 3-year overall survival (OS) rates were 89% (TAH-BSO alone) and 88% (TAH-BSO plus lymphadenectomy), and 3-year relapse-free survival (RFS) was even better in the TAH-BSO alone arm (hazard ratio [HR] 1.35, p = .017; HR 1.25 after adjustment, p = .14). An Italian randomized trial comparing TAH-BSO with lymphadenectomy with TAH-BSO alone for stage I endometrial carcinoma confirmed these results, with a median of 30 nodes removed in the patients in the lymphadenectomy study arm.114 Although the rate of nodal involvement was 13% in the lymphadenectomy arm as compared with 3% in the standard arm, rates of disease-free survival (DFS), OS, and relapses were the same in both arms. Even the pattern and sites were very similar, with vaginal recurrences in 2.6% versus 2.4% and lymph node recurrences in 1.5% versus 1.6% of patients in the lymphadenectomy versus standard study arms.114 Although many U.S.-based gynecologic oncologists continue to advocate for nodal staging in low-risk patients despite these results from randomized trials, the data do not support the routine use of lymphadenectomy for patients with stage I endometrial carcinoma.
Two randomized trials investigating the role of lymphadenectomy in clinical stage I endometrial cancer have recently been published. In the U.K. Medical Research Council ASTEC trial 1408 patients were randomized, 704 to TAH-BSO with lymphadenectomy and 704 to TAH-BSO alone.113 The baseline characteristics were well balanced between the groups: 9% had any nodal involvement. The results showed no benefit of lymphadenectomy: 3-year overall survival (OS) rates were 89% (TAH-BSO alone) and 88% (TAH-BSO plus lymphadenectomy), and 3-year relapse-free survival (RFS) was even better in the TAH-BSO alone arm (hazard ratio [HR] 1.35, p = .017; HR 1.25 after adjustment, p = .14). Subgroup analysis did not reveal any subgroup benefiting from lymphadenectomy. Analysis of the impact of the number of nodes removed was done by comparing centers with median node counts greater than 10 versus those with 10 or less and those with counts greater than 15 versus those with 15 or less. In both of these comparisons there was no difference between the study arms, with a nonsignificant trend in regression-free survival favoring the TAH-BSO alone arm. More women in the lymphadenectomy study arm had moderate or severe complications (17% vs. 12%; moderate to severe lymphedema 3.5% vs. 0.003%).113 An Italian randomized trial comparing TAH-BSO with lymphadenectomy with TAH-BSO alone for stage I endometrial carcinoma confirmed these results, with a median of 30 nodes removed in the patients in the lymphadenectomy study arm.114 Although the rate of nodal involvement was 13% in the lymphadenectomy arm as compared with 3% in the standard arm, rates of disease-free survival (DFS), OS, and relapses were the same in both arms. Even the pattern and sites were very similar, with vaginal recurrences in 2.6% versus 2.4% and lymph node recurrences in 1.5% versus 1.6% of patients in the lymphadenectomy versus standard study arms.114 Although many U.S.-based gynecologic oncologists continue to advocate for nodal staging in low-risk patients despite these results from randomized trials, the data do not support the routine use of lymphadenectomy for patients with stage I endometrial carcinoma. Subsequent therapy in the ASTEC trial was not determined by the lymph node status found at time of surgery, and the trial therefore tested the therapeutic value of lymphadenectomy per se, not whether any subsequent treatment based on lymph node status could affect outcomes. In the Italian trial, the use of adjuvant therapy was not significantly different between the study arms; the rates of patients receiving radiation therapy, chemotherapy, or both were 17%, 9%, and 6% in the lymphadenectomy study arm and 25%, 6%, and 4% in those who did not have lymphadenectomy. Ten of 59 patients received extended-field radiation therapy (EFRT) in the lymphadenectomy group versus 5 of 74 who did not have lymph nodes removed. There was, however, no difference in rates of total (12.8% vs. 13.2%), intraperitoneal (3% vs. 2.8%), or other relapses.114
Sentinel node detection may be an alternative way to identify patients requiring more intensive therapy. Initial results from sentinel node studies in endometrial carcinoma have shown that the combined use of radiocolloid labeling and patent blue dye results in sentinel node detection rates of 82% to 94%, with identification of two or three sentinel nodes per patient.50,51,115 The sentinel nodes were located in the obturator, external iliac, or para-aortic regions. In the study by Barranger and associates,49 macrometastases were identified in three sentinel nodes from two patients with routine staining, and immunohistochemical analysis identified six additional micrometastatic sentinel nodes in three other patients and one sentinel node containing isolated tumor cells. No false-negative sentinel nodes were found. Increasing surgical volume (and operator experience) has been shown to be associated with increased detection rates (77% vs. 94% after at least 30 cases).116 Additional larger studies are needed to further explore this concept, establish optimal techniques, and develop reliable accuracy data.111,117
Sentinel node detection may be an alternative way to identify patients requiring more intensive therapy. In breast cancer it has been shown that removal and meticulous analysis of sentinel nodes with serial sectioning and immunohistochemistry more adequately identifies occult nodal involvement while sparing most patients the risks and added toxicities of more extensive procedures. Initial results from sentinel node studies in endometrial carcinoma have shown that the combined use of radiocolloid labeling and patent blue dye results in sentinel node detection rates of 82% to 94%, with identification of two or three sentinel nodes per patient.50,51,115 The sentinel nodes were located in the obturator, external iliac, or para-aortic regions. In the study by Barranger and associates,49 macrometastases were identified in three sentinel nodes from two patients with routine staining, and immunohistochemical analysis identified six additional micrometastatic sentinel nodes in three other patients and one sentinel node containing isolated tumor cells. No false-negative sentinel nodes were found. Increasing surgical volume (and operator experience) has been shown to be associated with increased detection rates (77% vs. 94% after at least 30 cases).116 Additional larger studies are needed to further explore this concept, establish optimal techniques, and develop reliable accuracy data.111,117
Primary Radiation Therapy: Indications and Results
Several studies have demonstrated the efficacy of primary RT for clinical stage I disease. With the use of uterine brachytherapy with or without EBRT, 5-year uterine control rates of 70% to 90% and disease-free survival rates ranging from 50% to 80% have been reported.118–124 Grade 3 tumors had significantly lower pelvic control and survival rates than grade 1 or 2 disease. Studies that included patients with stage II disease reported 5-year pelvic control rates of 40% to 60% and DSS of 50% to 60%.120,124
Surgical Results: Early-Stage Disease
Many retrospective studies have reported invariably good outcomes for stage IA and IB grade 1 and 2 endometrioid carcinoma treated with TAH-BSO alone, with a 5-year RFS of 95% and 5-year vaginal relapse rates of 2% to 5%.125–128 Several investigators stressed that lymphadenectomy is not indicated in these low-risk patients.127,128 In some studies, vaginal brachytherapy was used.128 The addition of brachytherapy to TAH-BSO may reduce vaginal relapse rates from between 2% and 5% to between 0% and 2% but without a survival difference and at the cost of (albeit minimal) morbidity and procedural cost. Effective salvage treatment is available for the occasional patient with vaginal relapse.
Adjuvant Therapy: Stages I and II
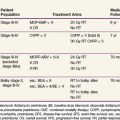
Four prospective, randomized trials have been published that evaluated the role of postoperative pelvic irradiation in intermediate-risk endometrial carcinoma,74–76129 and they are summarized in Table 57-7. The Norwegian trial, published in 1980, included 540 women with clinical stage I endometrial carcinoma. After hysterectomy and postoperative vaginal brachytherapy (60 Gy to the mucosal surface), patients were randomly assigned to additional pelvic irradiation (40 Gy in 2-Gy fractions, with a midline block after 20 Gy) or observation. Although additional pelvic irradiation reduced vaginal and pelvic relapse rates (2% at 5 years vs. 7% in the control group), more distant metastases were found in the pelvic irradiation group (10% vs. 5%), and survival was not improved (89% vs. 91% at 5 years).74 The subgroup with grade 3 tumors and deep (>50%) myometrial invasion showed improved local control and survival after pelvic irradiation (18% vs. 27% cancer-related deaths); however, there were too few patients in this category to reach significance.
TABLE 57-7 Comparison of the Randomized Trials of Adjuvant Radiation Therapy for Stage I Endometrial Carcinoma
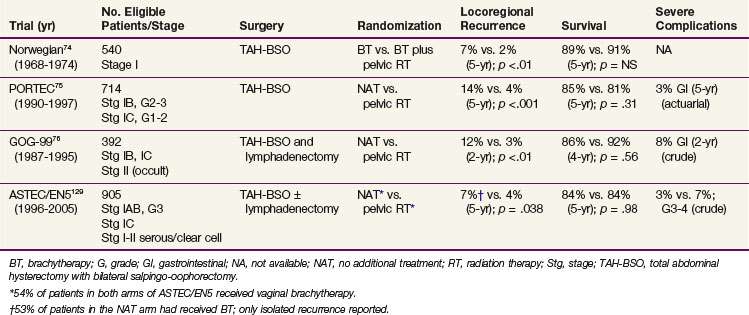
In the Postoperative Radiation Therapy in Endometrial Carcinoma (PORTEC) trial, 715 patients with stage I endometrial carcinoma, grade 1 or 2 with deep (>50%) myometrial invasion or grade 2 or 3 with superficial (≤50%) invasion were randomized after TAH-BSO to receive pelvic radiation therapy (46 Gy in 2-Gy fractions) or no further treatment.75 The 10-year locoregional relapse rates were 5% in the radiation therapy group and 14% in the control group (p <.0001). There was no significant survival difference between the treatment arms with 10-year OS of 66% (irradiation) and 73% (controls; p = .09).130 Endometrial cancer-related death rates were 10% in the RT group and 8% in the control group (p = .47). The patients younger than age 60 years (both study arms) had a 5-year locoregional relapse rate of 3%, compared with 9% for patients 60 to 70 years old and 10% for those older than 70 years. Patients with grade 2 tumors with superficial invasion had a 5-year locoregional relapse rate of 5%. Risk criteria for relapse were grade 3, age older than 60 years, and outer 50% invasion.
The 5-year survival rate after any relapse was 13% in the RT group and 48% in the control group (p <.001). After vaginal relapse, 5-year actuarial survival rates were 38% in the RT group and 70% in the control group, which shows the high salvage rates of vaginal relapse in patients not previously irradiated. Most (87%) of the 39 patients with isolated vaginal relapse could be treated with curative intent, usually with pelvic EBRT and brachytherapy (BT) and with surgery in some. A complete remission was obtained in 89%, and 77% remained in complete remission after further follow-up.131 In contrast, only 4 of 10 patients who were treated for pelvic relapse reached a complete remission, and the outcome after pelvic and distant relapse was poor, with only 6% and 11% of patients, respectively, surviving 5 years.
The GOG-99 trial included 392 evaluable patients with stage IB, IC, or IIA endometrial carcinoma of any histologic grade who were randomized after TAH-BSO and lymphadenectomy to receive pelvic irradiation (50.4 Gy in 1.8-Gy fractions) or no additional treatment.76 A high-intermediate risk group was defined based on the prognostic factors of age, histologic grade, myometrial invasion, and the presence of LVSI. This group (33% of the study population) had a 2-year incidence of relapse in the no additional treatment arm of 27%, in contrast to 6% for the low-intermediate risk group (67% of patients). Radiation therapy resulted in similar hazard reductions for the high- and low-intermediate risk subgroups (58% and 54%), but in absolute terms the differences were greater for the high-intermediate risk patients, with a reduction of 4-year cumulative relapse from 27% (in the group with no additional treatment) to 13% (those with irradiation). There was even a slight, although nonsignificant survival benefit: 4-year OS was 86% for the no additional treatment group and 92% for those who had RT. The 2-year estimated vaginal and pelvic failure rate was 12% in the no additional treatment group and 3% in the RT group, for a 58% hazard reduction by irradiation. These results are strikingly similar to those obtained in the PORTEC study without lymphadenectomy. However, the 4-year crude rate of severe complications in GOG-99 was 13% for patients who had received irradiation, compared with a 5-year actuarial rate of 3% in the PORTEC trial, which underlines the increased risk of toxicity when combining extended surgery with nodal sampling or dissection with pelvic RT.
The multicenter randomized ASTEC/EN5 trial included 905 patients with stage I-IIA endometrial carcinoma with risk features (deep invasion or grade 3 with superficial invasion or serous histology), who were randomly allocated to EBRT or observation. Brachytherapy was permitted if used in both study arms, and 53% of the patients received BT. Again, there was no difference in OS (84% at 5 years in both groups).129
A meta-analysis of pooled data from the ASTEC/EN5, GOG-99, and PORTEC-1 trials, which updated the 2007 Cochrane review and meta-analysis132 with the ASTEC/EN5 data, reliably excluded an absolute survival benefit of pelvic RT of more than 3%. The hazard ratio for isolated vaginal or pelvic RFS was 0.46 (p = .02), with 5-year cumulative incidence rates of 6.1% (observation only) versus 3.2% (RT). The relatively low rate of isolated vaginal or pelvic recurrence can probably be explained by the fact that 53% of the patients in the observation study arm received vaginal BT.129
Conclusions that can be drawn from these randomized trials of pelvic RT in stage I endometrial carcinoma are that pelvic irradiation provides a highly significant improvement of local control but offers no survival advantage. A large proportion of endometrial cancer patients has a very favorable prognosis, and these patients should be observed after TAH-BSO. Radiation therapy is a very effective salvage treatment for vaginal relapse in patients not previously irradiated. The data suggest that the use of postoperative RT should be limited to the group of patients at sufficiently high risk for locoregional relapse to accept the risk of treatment-associated morbidity to maximize initial local control and RFS. This has led to a reduction of the use of pelvic EBRT and use of high-intermediate risk criteria to determine the indication for radiation therapy. In the PORTEC study, patients with two of the three major risk factors (grade 3, age 60 or older, and outer 50% myometrial invasion) were found to have the highest absolute benefit from pelvic irradiation. The 10-year locoregional relapse rates in this “high-intermediate risk” category were 5% in the radiation therapy group and 20% in the control group. In the GOG-99 trial, similar high-intermediate risk criteria were identified, with reduction of isolated 4-year local relapse in the high-intermediate risk group from 13% to 5%. The risk criteria as defined in the PORTEC and GOG-99 trials and the risk reduction with radiation therapy in the high-risk groups are listed in Table 57-8.
TABLE 57-8 Comparison of the Risk Groups in the PORTEC and GOG-99 Trials and Risk Reduction with Radiation Therapy
| Risk Levels | Risk Groups | |
|---|---|---|
| PORTEC75 | GOG-9976 | |
| Risk factors | ||
| Age | ≤60 vs. >60 | ≤50 vs. ≤70 vs. >70 |
| Grade | Grade 1-2 vs. 3 | Grade 1 vs. 2-3 |
| Deep invasion | ≤50% vs. >50% | ≤66% vs. >66% |
| Lymphovascular space invasion | Absent vs. present | |
| High-risk group | At least two of the three factors | Any age and three factors |
| Age ≥50 and two factors | ||
| Age ≥70 and one factor | ||
| Results for the high-risk group | 10-yr locoregional relapse | 4-yr relapse (any) |
| RT: 5% | RT: 13% | |
| NAT: 23% | NAT: 27% | |
| Rel. risk: 0.22 | Rel. risk: 0.48 | |
| With GOG high-risk criteria | 4-yr isolated local relapse | |
| RT: 8% | RT: 5% | |
| NAT: 22% | NAT: 13% | |
| Rel. risk: 0.36 | Rel. risk: 0.38 | |
GOG, Gynecologic Oncology Group; NAT, no additional treatment; PORTEC, Postoperative Radiation Therapy in Endometrial Carcinoma; Rel. risk, relapse with RT compared with NAT; RT, radiation therapy.
Because most relapses occur in the vagina, the use of vaginal BT alone has been advocated, especially after extensive surgical staging. Data from mostly retrospective studies that used vaginal brachytherapy alone for stage I endometrial cancer have shown the 5-year risk of vaginal relapse to be 0% to 7%.133–141 Pelvic and distant failure rates, however, remain similar to those of patients treated with surgery alone, which is the reason that most studies included only or mainly low-risk patients (i.e., grade 1 to 2 disease with no or superficial invasion).
Vaginal control and complication rates for high-dose-rate (HDR) vaginal BT are comparable to those of low-dose-rate (LDR) therapy.137 Petereit and Pearcey142 reviewed the results of HDR BT for stage I endometrial cancer patients and concluded that local control rates of 98% and higher were obtained with modest doses (e.g., 30-35 Gy HDR to the surface or 21 Gy to 5-mm depth in three fractions). The use of higher doses did not further increase local control, but complication rates were higher. Several HDR studies using surgical staging included patients with high-risk stage I or stage II disease and reported vaginal control rates of 98% to 100%. Pelvic and distant relapses were found mainly in the stage I or II patients with high-risk features.138–141
The results of the randomized trials for intermediate-risk endometrial carcinoma suggested that, in view of the absence of survival benefit with EBRT and of the fact that most recurrences were located in the vagina, vaginal BT might also be effective for patients with high-intermediate risk features to obtain local control with fewer side effects than EBRT and better quality of life. This was the rationale for the randomized PORTEC-2 trial (2002-2006), which compared EBRT and vaginal BT with regard to both efficacy and health-related quality of life. In the PORTEC-2 trial, 427 patients with stage FIGO 1988 stage I-IIA endometrial carcinoma with high-intermediate risk features (i.e., age of at least 60 years, grade 1 or 2 tumors with outer 50% invasion or grade 3 with inner 50% invasion) were randomly assigned after surgery (TAH-BSO without lymphadenectomy) to EBRT (n = 214) or vaginal brachytherapy (n = 213). Quality of life was significantly better in the patients in the vaginal BT arm. Patients who had brachytherapy reported better social functioning (p <.002) and lower symptom scores for diarrhea, fecal leakage, the need to stay close to the toilet, and limitation in daily activities due to bowel symptoms (p <.001). At baseline, 15% of patients were sexually active; this increased significantly to 39% during the first year (p <.001). Sexual functioning and symptoms did not differ between the treatment arms.143 Final results of the PORTEC-2 trial confirmed the efficacy of vaginal brachytherapy. At median follow-up of 45 months, estimated 5-year rates of vaginal recurrence were 1.8% for VBT and 1.6% for EBRT (p = .74). Five-year rates of locoregional relapse (vaginal recurrence and/or pelvic recurrence) were 5.1% and 2.1% (p = .17). Only 1.5% versus 0.5% (p = .30) presented with isolated pelvic recurrence; other pelvic recurrences were part of widespread disease relapse, whereas rates of distant metastases were similar (8.3 vs. 5.7%, p = .46). There were no differences in OS (84.8% vs. 79.6%, p
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


