The external ear consists of the auricle or pinna, the external auditory meatus (canal), and the tympanic membrane (Fig. 13-1). The external auditory canal (EAC) connects the tympanic membrane to the exterior and is approximately 2.4 cm long. The outer third is cartilaginous, whereas the inner two thirds is bony and slightly narrower. The tympanic membrane, made of multiple layers of squamous epithelium, separates the auditory canal from the middle ear (6).
The tympanic (or middle ear) cavity houses the auditory ossicles and opens into the eustachian tube to communicate with the pharynx. The overall length of the eustachian tube is 3.5 cm.
The inner or internal ear lies in the petrous portion of the temporal bone and consists of the bony labyrinth and the membranous labyrinth.
The acoustic nerve, arising at the lateral termination of the internal acoustic meatus and ending in the brainstem between the pons and the medulla, is responsible for auditory and vestibular function.
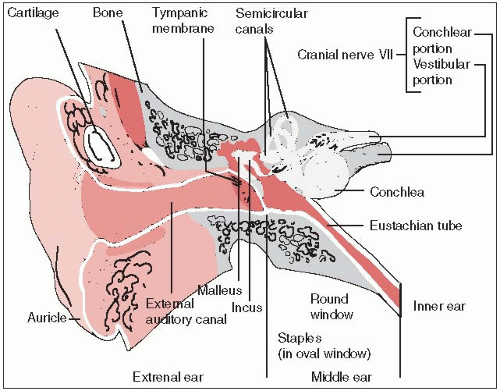 FIGURE 13-1 Anatomy of the ear. |
Lymphatic vessels of the tragus and anterior external portion of the auricle drain into the superficial parotid lymph nodes. Lymphatic vessels of the posterior-external and whole-cranial aspect of the auricle drain into the retroauricular lymph nodes, whereas those of the lobule drain into the superficial cervical group of lymph nodes.
Lymphatics from the middle ear and the mastoid antrum pass into the parotid nodes and the upper deep cervical lymph nodes.
The lymphatics in the middle ear and eustachian tube are sparse; the inner ear has no lymphatics.
Tumors present as small ulcerations, mostly on the helix.
Pruritus and pain are common for lesions of the EAC.
High-resolution computed tomography can help determine the operability of tumors (9).
Magnetic resonance imaging (MRI) can sometimes provide excellent delineation of soft-tissue tumor margins, muscle infiltration, intracranial extension, and vessel encasement.
Diagnosis is always established by biopsy.
Approximately 85% of tumors involving the auditory canal, middle ear, and mastoid area are squamous cell carcinomas, while the majority of cancers of the sun-exposed pinna are basal cell carcinomas.
Large lesions involving the middle ear and lesions with extension into the temporal bone are usually the most difficult to treat.
Seventh nerve palsy associated with middle ear tumors indicates poor local control.
Neither the American Joint Committee nor the International Union Against Cancer has a staging system for tumors of the ear.
Arriaga et al. (3) have proposed a staging system for carcinoma of the EAC based on clinical and radiographic findings (Table 13-1). Tumors of the pinna are typically staged according to the AJCC staging system for skin cancers (see Table 9-1).
Tumors of the auricle are most often treated with limited surgery or external radiation therapy.
Irradiation treatment in early stages is usually with orthovoltage or electron beam therapy (10).
TABLE 13-1 Proposed Staging System for Tumors of the EAC (Pittsburgh System) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
Most techniques have been fairly successful in the treatment of lesions in this area.
Surgery is beneficial if the lesion has invaded the cartilage of the ear or extends medially into the auditory canal.
Afzelius et al. (1) indicated that lesions over 4 cm, as well as those with cartilage invasion, have an increased risk of nodal spread. Prophylactic neck dissection is recommended (2).
Interstitial irradiation using afterloading192Ir, particularly for tumors smaller than 4 cm, is also an effective method of treatment, affording excellent local control with good cosmesis (9).
Lesions of the outer part of the auditory canal require local excision with a margin of at least 1 cm between the lesion and the tympanic membrane if there is no radiographic evidence of invasion of the mastoid.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


