those with a palpable mass, 47.1% also had mammographic abnormalities. Microcalcification was the most common finding in 75.5%, with fine pleomorphic calcifications being the most frequently seen (40.4%), followed by amorphous or indistinct calcifications (35.9%). Fine pleomorphic and finelinear branching calcifications were significantly associated with the presence of grade 3 DCIS and necrosis (13).
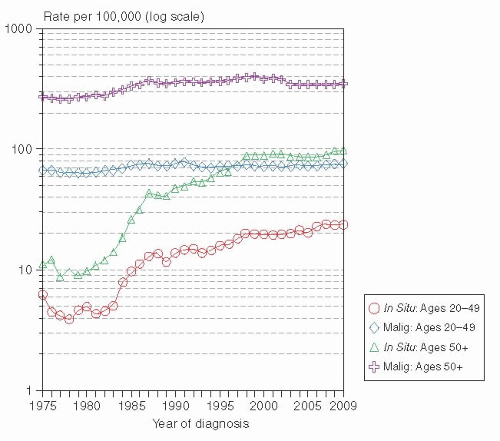 FIGURE 23-1 SEER Incidence rates 1975 to 2009 for in situ versus invasive breast cancer by age, all races. (From Howlader N, Noone AM, Krapcho M, et al., eds. SEER Cancer Statistics Review, 1975-2010, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2010/, based on November 2012 SEER data submission, posted to the SEER web site, April 2013.) |
differentiation: 90% of poorly differentiated cases grew in a continuous manner without gaps, while 45% and only 30% of intermediate and well-differentiated lesions, respectively, were continuous. The findings in these two studies indicate that, in most cases, DCIS involves the breast in a segmental distribution, and truly multicentric disease is uncommon.
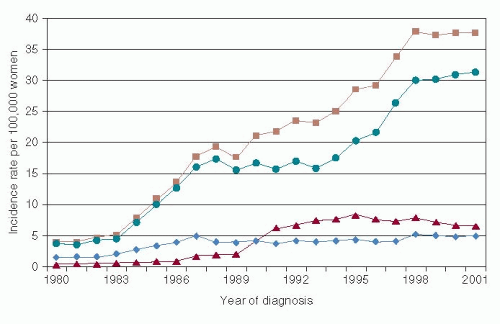 FIGURE 23-2 Incidence of in situ carcinoma (per 100,000 women) by different histological types among women ages ≥ 30 years, 1980 to 2001. (▪ DCIS overall, • non-comedo DCIS, ▲ comedo DCIS, ♦ LCIS. From Li CI, Daling JR, Malone KE, et al. Age-Specific Incidence Rates of In situ Breast Carcinomas by Histologic Type, 1980 to 2001. Cancer Epidemiol Biomarkers Prev. American Association for Cancer Research, 2005). |
DCIS, and 80% of comedo DCIS lesions. This observation that the majority of both comedo and non-comedo DCIS share their LOH phenotypes with synchronous invasive breast cancer supports the concept that DCIS is a direct precursor of invasive breast cancer.
TABLE 23-1 Recurrences after Mastectomy for DCIS (recent series with >100 cases and >5 years follow-up) | ||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||
TABLE 23-2 Radiotherapy Effect: Results of the Phase III Randomized Control Trials | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 23-3 Patient and Treatment Variables in the Phase III Randomized Control Trials Evaluating Radiotherapy Effect Post Lumpectomy for DCIS | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
average annual reduction in ipsilateral breast cancer events was demonstrated with the addition of radiotherapy after lumpectomy (38) that persisted at 8 (39)and 12 years median follow-up (40). The most recent analysis done after 17.25 years median follow-up demonstrates a sustained benefit of breast radiotherapy with a 52% relative reduction in the risk of invasive ipsilateral breast cancer recurrence (hazard ratio [HR], 0.48; 95% CI, 0.33-0.69; p < .001) and a 47% reduction in the risk of DCIS ipsilateral in-breast recurrence (HR, 0.53; 95% CI, 0.35-0.8; p < .001) compared to those randomized to lumpectomy alone. The same percentage of women developed contralateral breast cancer in the lumpectomy-alone group (10.3%) and in the group that received radiotherapy (10.2%). Likewise, overall and breast cancer mortality did not differ for the lumpectomy-alone versus the breast radiotherapy group (2).
(45). The eligibility criteria for RTOG 9804 are similar to the low/intermediate-grade stratum of the Eastern Cooperative Oncology Group (ECOG) single arm registration-observation study for DCIS post lumpectomy discussed elsewhere (46). For the low/intermediate-grade stratum on ECOG 5194, the 7-year rate of ipsilateral breast recurrence is 10.5% (46). This discrepancy in 7-year rates of ipsilateral breast recurrence between the two trials may be influenced by the tamoxifen use that was double in the RTOG 9804 (62%) population compared to the ECOG 5194 low/intermediate-grade stratum (31%). Additional follow-up of RTOG 9804 is needed to ensure endurance of the results given its incomplete accrual and the longer time to failure that has been reported for lower-grade DCIS; however, it appears that, based on standard clinical-pathologic criteria, a cohort of DCIS could be identified with a low rate of in-breast recurrence at 7 years without radiotherapy (but with tamoxifen in most). However, even in this low-risk group, the addition of radiotherapy reduced the in-breast recurrence rate by a relative 89% and an absolute 5.8%.
TABLE 23-4 Outcome for DCIS Treated with Lumpectomy and Whole Breast Radiotherapy from Single- and Multi-Institution Experiences | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 23-5 Breast Radiotherapy Delivered in Randomized Control Trials Evaluating Benefit after Lumpectomy for DCIS | ||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
York University reported a Phase I/II single arm prospective trial in 59 patients using hypofractionated WBI of 42 Gy in 15 fractions of 2.8 Gy for treatment of DCIS (48). At a median follow-up of 36 months, there were no grade 3 radiation toxicities early or late, 91% of women reported a good-excellent cosmetic outcome, and no in-breast recurrences were reported. The University of Toronto reported their retrospective analysis of 266 women with DCIS who received either standard fractionated (104 cases) or hypofractionated (162 cases) WBI post lumpectomy. With a median follow-up of 3.76 years, the actuarial risk of ipsilateral breast recurrence at 4 years was 7% with hypofractionated WBI and 6% with the conventional schedule (p = .9) (49). The American Society for Radiation Oncology (ASTRO) evidence-based guideline on Fractionation for Whole Breast Irradiation concluded that data were insufficient so far to recommend for or against hypofractionated WBI post lumpectomy for women with DCIS (50).
cancer events in the tamoxifen group than the placebo group (p = .0009). A lower rate of ipsilateral-breast recurrences in the tamoxifen group was apparent only for invasive tumors (44% reduction). The rate of ipsilateral DCIS recurrences was not significantly lower in the tamoxifen group (p = ·43), but the reduction in contralateral breast DCIS was 13 versus 3, a 78% reduction (p = .02). Long-term outcomes of NSABP B-24 reporting at a median follow-up of 13.6 years (2) demonstrate a sustained 32% reduction in the risk of invasive ipsilateral recurrence in the tamoxifen compared with the placebo group (HR, 0.68; 95% CI, 0.49-0.95; p = .025). Regarding ipsilateral DCIS recurrences, the addition of tamoxifen resulted in a non-statistically significant risk reduction of 16% compared with placebo (HR, 0.84; 95% CI, 0.60-1.19; p = .33). There was a 32% reduction in contralateral breast cancer for patients who received tamoxifen versus placebo (HR, 0.68; 95% CI, 0.48-0.95; p = .023).
radiotherapy to determine whether trastuzumab given concurrently with radiotherapy is beneficial in preventing subsequent breast cancer events. The targeted accrual is 2,000, and as of the close of 2012, over 1,000 patients have been randomized.
TABLE 23-6 Results of Treatment of Ductal Carcinoma In Situ with Excision Alone, Retrospective Series | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:
 Breast Cancer Screening
Breast Cancer Screening
 Ductal Carcinoma In Situ and Other Intraductal Lesions: Pathology, Immunohistochemistry, and Molecular Alterations
Ductal Carcinoma In Situ and Other Intraductal Lesions: Pathology, Immunohistochemistry, and Molecular Alterations
 Adjuvant Systemic Therapy: Endocrine Therapy
Adjuvant Systemic Therapy: Endocrine Therapy
 Preoperative Endocrine Therapy for Operable Breast Cancer
Management Summary for the Care of Patients with Metastatic Breast Cancer
Nursing Care in Patient Management and Quality of Life
Preoperative Endocrine Therapy for Operable Breast Cancer
Management Summary for the Care of Patients with Metastatic Breast Cancer
Nursing Care in Patient Management and Quality of Life
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


