DIFFERENTIAL DIAGNOSIS OF THYROID NODULES
Part of “CHAPTER 39 – THE THYROID NODULE“
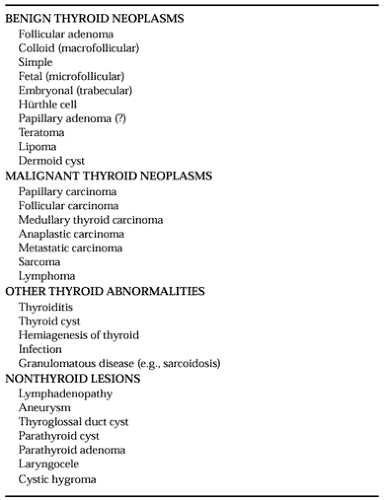
The differential diagnosis of apparent thyroid nodules covers a wide range of pathology1,2,3,4 and 5 (Table 39-1). The usual diagnostic challenge is to distinguish malignant from benign lesions. Most true intrathyroidal nodules are colloid adenomas (27–60%) or simple follicular adenomas (26–40%), although fully reliable figures are not available.18 Follicular adenomas introduce significant uncertainty in the diagnosis and treatment
because no available measures short of surgical resection with detailed histologic examination allow the separation of well-differentiated follicular carcinomas from adenomas. Instead, the distinction depends on the presence or absence of capsular or vascular invasion by the tumor; cellular detail is of little value.19 Hürthle cell tumors are a subset of follicular lesions composed of oval to polygonal cells with dense, granular, acidophilic cytoplasm and a prominent macronucleolus. The malignant potential of histologically benign Hürthle cell tumors and the natural history of Hürthle cell malignancies continue to be subjects of controversy.20,21
because no available measures short of surgical resection with detailed histologic examination allow the separation of well-differentiated follicular carcinomas from adenomas. Instead, the distinction depends on the presence or absence of capsular or vascular invasion by the tumor; cellular detail is of little value.19 Hürthle cell tumors are a subset of follicular lesions composed of oval to polygonal cells with dense, granular, acidophilic cytoplasm and a prominent macronucleolus. The malignant potential of histologically benign Hürthle cell tumors and the natural history of Hürthle cell malignancies continue to be subjects of controversy.20,21
 |
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


