DEVELOPMENTAL ENDOCRINOLOGY
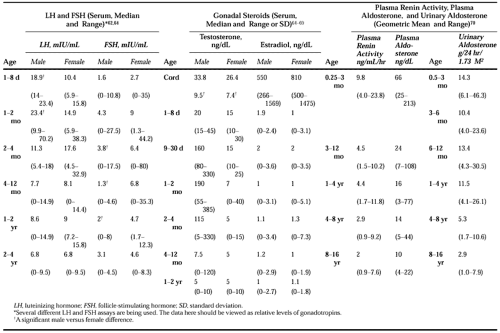
The pediatric patient undergoes continuous change that is reflected not only in growth rates but also in the secretory activity of the endocrine system. The perinatal period is one of rapid change in the endocrine system when the child is adjusting to extrauterine life (Table 7-6). This is further complicated by the differences that may exist in hormonal levels in the full-term versus preterm infant. This section outlines some of these hormonal variations. As a general rule, one can divide the analysis of hormonal secretory activity into the following developmental periods: fetal, perinatal, childhood, and pubertal.50,51
 |
GROWTH HORMONE AND INSULIN-LIKE GROWTH FACTORS
Immunoreactive growth hormone is found in human anterior pituitary glands as early as the seventh week of gestation.49 Pituitary growth hormone increases from 0.44μg per gland at 10 to 14 weeks of gestation to a mean of 675μg per gland at term. However, pituitary growth hormone level is fairly constant after 25 weeks of gestation. Growth hormone is also detectable in fetal serum in high concentration. These high concentrations of growth hormone may be a reflection of hypothalamic-pituitary neuroendocrine immaturity. At 10 to 14 weeks of gestation, the mean growth hormone level in fetal serum is 65 ng/mL, and it rises rapidly to a peak fetal concentration of 132 ng/mL at 20 to 25 weeks of gestation. Thereafter, serum growth hormone declines to 35 ng/mL at 35 to 40 weeks of gestation.
The postulated immature neuroendocrine control of growth hormone secretion persists into the neonatal period. Growth hormone is not suppressed by glucose until 1 month of age, and the normal sleep-induced rise in serum growth hormone levels does not appear until 3 months of age.51
Insulin-like growth factor-I (IGF-I) plasma concentrations show a marked age-related pattern. The normal ranges, as reported by the Quest Diagnostic Nichols Institute, are shown in Figure 7-8 and Figure 7-9. The range is large, and a marked overlap of values is seen when one compares the lower range of normal with values typically associated with growth hormone deficiency. Plasma IGF-I levels increase with age; during puberty concentrations are reached that would be associated with acromegaly if encountered in an adult. After puberty, the levels decline to the normal adult range. Females generally have IGF-I levels ˜20% higher than those of males. The normal level of IGF-I may correlate better with the child’s physiologic development. Such a relation is seen during puberty (see Fig. 7-9). For prepubertal boys, a similar relation with bone age may be valid as well.52,53 Insulin-like growth factor–binding protein-3 (IGFBP-3) has been suggested as another serum protein reflective of growth hormone secretion and function.54 In a manner similar to IGF-I, normal values for IGFBP-3 vary according to age and stage of puberty (Fig. 7-10).
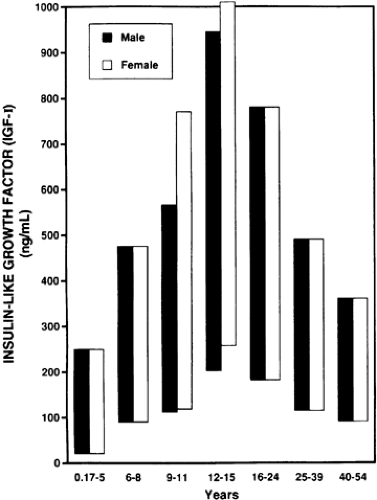 FIGURE 7-8. Variation of insulin-like growth factor-I with age and sex. (Data derived from the normal values provided by Quest Diagnostic Nichols Institute, San Juan Capistrano, California.) |
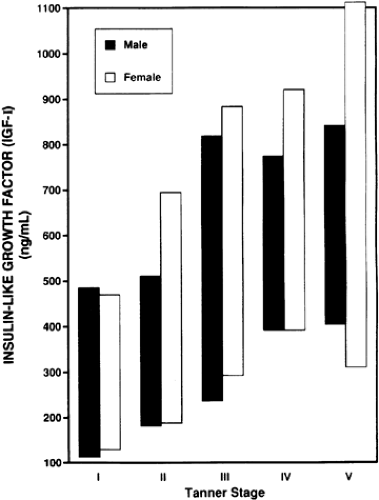 FIGURE 7-9. Variation of insulin-like growth factor-I with stage of puberty and sex. (Data derived from the normal values provided by Quest Diagnostic Nichols Institute, San Juan Capistrano, California.) |
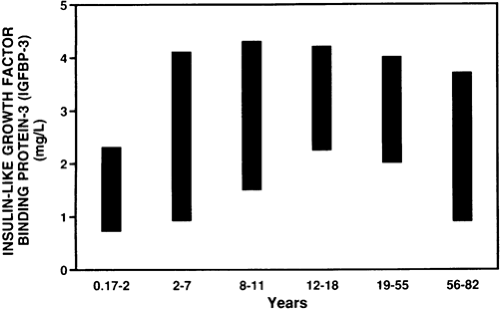 FIGURE 7-10. Variation of insulin-like growth factor–binding protein-3 with age. (Data derived from the normal values provided by Quest Diagnostic Nichols Institute, San Juan Capistrano, California.)
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
