Coumarin-Induced Skin Necrosis and Venous Limb Gangrene
Coumarin-Induced Skin Necrosis and Venous Limb Gangrene
Theodore E. Warkentin
Thrombotic events that result from coumarin administration are incongruous but well-documented complications of anticoagulant therapy. The key role of coumarin (vitamin K antagonist) in causing thrombosis and necrosis is by the depletion of one or both vitamin K-dependent natural anticoagulants, protein C, and protein S. In this chapter, coumarin-induced necrosis denotes both (central) skin necrosis and (acral) venous limb gangrene syndromes. Coumarin-induced skin necrosis (CISN) was first recognized by Verhagen,1 who described 13 cases in 1954, noting features such as its female predominance, characteristic localization of lesions, and typical onset within a few days of initiating coumarin. CISN is characterized by infarction and necrosis of the skin and underlying subcutaneous tissues.2, 3 A distinct though related syndrome, coumarin-induced venous limb gangrene, is linked to warfarin treatment of acute deep vein thrombosis (DVT) complicating certain hypercoagulability disorders, most notably immune heparin-induced thrombocytopenia (HIT) and adenocarcinoma.4, 5, 6, 7, 8, 9, 10, 11
COUMARINS
The coumarins are a group of naturally occurring lactones that are produced by a number of plants and microbes. Ironically, the least complex member, coumarin (1,2-benzopyrone), has no anticoagulant action despite its synonymous designation for those chemically related molecules that possess anticoagulant activity.12 Warfarin (Coumadin), a 4-hydroxycoumarin derivative, is the most widely used oral anticoagulant in North America and worldwide.2 Therefore, most instances of CISN in North America are warfarin induced. However, the syndrome can be caused by other coumarin congeners (e.g., phenprocoumon, acenocoumarol, and nicoumalone), as well as by the rarely used phenindione group of oral anticoagulants.13, 14 Phenprocoumon (Marcumar) is widely used in continental Europe. Because its half-life is longer than that of warfarin (6 vs. 1.5 days), relatively large loading doses are often given; however, whether these differences result in a lesser or greater frequency of CISN, compared with warfarin, is unknown. The coumarins interfere with vitamin K epoxide reductase,15 producing posttranslational modifications of four procoagulant and two anticoagulant vitamin K-dependent factors16 (see Chapter 106).
PATHOGENESIS
Several observations suggest that the fundamental pathobiology of coumarin necrosis is a transient disturbance in procoagulant/anticoagulant balance that leads to microthrombosis in susceptible tissue sites. First, coumarin necrosis has a characteristic temporal profile, usually occurring within 1 week of initiating oral anticoagulant therapy.5, 6, 7, 9, 17, 18, 19, 20 During this interval, functional levels of protein C decline much more quickly than the major procoagulant factor, prothrombin,21, 22 because of differences in their half-lives16 (see Table 109.1); given that prothrombin inhibits the ability of activated protein C to inactivate factor Va,23 this early discrepancy in prothrombin versus protein C concentrations— (low-)normal and very low, respectively—can impair the protein C anticoagulant system. Second, the pathology is that of noninflammatory, small-vessel thrombosis affecting the dermal and subcutaneous postcapillary venules and small veins.5, 19 This is consistent with the role of the protein C anticoagulant pathway in preventing thrombosis of these small vessels.24 Third, a relatively high proportion of patients with CISN (although not with venous limb gangrene) have a hereditary abnormality of the protein C anticoagulant pathway, which predisposes such patients to further, potentially dangerous reductions in protein C during the first few days of oral anticoagulant treatment. Fourth, the clinical and pathologic appearance of CISN resembles that of neonatal purpura fulminans caused by severe congenital protein C deficiency.25 Fifth, skin necrosis can be a feature of acquired deficiency of protein C or protein S due to infection, autoimmunity, or the antiphospholipid syndrome26, 27, 28 or functional inhibition of protein C or protein S by antiphospholipid antibodies.29, 30 Sixth, coumarin necrosis (particularly venous limb gangrene) is associated with markedly increased thrombin generation.4, 5, 6, 31
COUMARIN-INDUCED SKIN NECROSIS
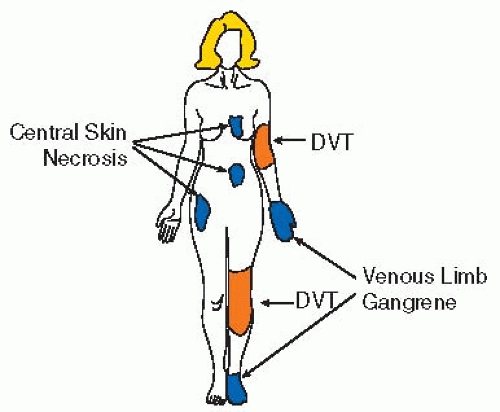
CISN refers to central (nonacral) necrosis of skin and subcutaneous tissues (see FIGURE 109.1) (4); it occurs more often in women (3:1 ratio), with mean age being 50 to 55 years, and most commonly involves sites with substantial underlying fatty tissues, such as the breast, anterior abdomen, buttocks, hips, thighs, and calves and less commonly, the flank, back, penis (ischemic priapism, necrosis), legs, arms, and face (e.g., cheeks, nose, eyelids, pinnae).3, 13, 17, 18, 19, 20, 32, 33, 34, 35, 36, 37, 38, 39 Multiple (sometimes symmetric) lesions are observed in about one-third of patients. CISN is rare (estimated frequency, 0.01% to 0.1%).3, 18
The typical temporal onset between 3 and 6 days of oral anticoagulant therapy occurs in 90% of patients,13, 17, 18, 19, 20, 40 although late onset after weeks or months has been reported.41, 42, 43 Localized pain, induration, and erythema progress over hours to central purplish black skin discoloration, usually with blistering, and ultimately evolving to well-demarcated, full-thickness necrosis of the skin and subdermal tissues (see FIGURE 109.2). With or without surgical debridement, there usually is a permanent region of depressed skin that reflects the loss of underlying tissues. The necrotic skin also presents the real possibility of secondary fatal sepsis.40, 42, 44
Table 109.1 Half-lives of the vitamin K-dependent procoagulant and anticoagulant factors
Procoagulant Factors
Half-Life, h
Anticoagulant Factors
Half-Life, h
Factor II (prothrombin)
60
Protein C
9
Factor X
40
Protein S
60
Factor IX
24
Factor VII
4-6
There are six vitamin K-dependent hemostatic factors: four with procoagulant activity and two with anticoagulant activity. Treatment with coumarin anticoagulants reduces functional levels of these factors. The paradoxic procoagulant effect of warfarin can be explained by the different half-lives16of these factors following the onset of action of coumarin—the time to a therapeutically significant reduction of the major procoagulant factor, prothrombin (half-life, ˜60 h), is much longer than the time to a clinically important reduction in the major anticoagulant factor, protein C (half-life, ˜9 h). Thus, within the first several days of coumarin anticoagulation, and under certain clinical circumstances (see text), there can arise a transient, but clinically important, disturbance in procoagulant—anticoagulant balance.
The earliest stages of CISN can resemble subcutaneous hemorrhage. Incipient skin necrosis is suggested by (a) recent initiation of coumarin, (b) typical location of lesions, (c) absence of trauma, and (d) an international normalized ratio (INR) that is within (in 33% to 60% of patients) or above the therapeutic range.17, 18 CISN that occurs when the INR is within the therapeutic range suggests that the patient has a preexisting abnormality of the protein C natural anticoagulant pathway, as noted in four family members with hereditary protein S deficiency.45 In contrast, when warfarin-induced venous limb gangrene complicates disorders associated with disseminated intravascular coagulation (DIC), such as HIT or adenocarcinoma, there typically is a supratherapeutic INR (>3.5). This reflects the special susceptibility of factor VII and protein C to severe depletion during coumarin therapy in DIC. In such patients, congenital abnormalities of the protein C natural anticoagulant pathway are usually not present.5, 6, 10, 44
FIGURE 109.1 Two syndromes of coumarin-induced necrosis. (a) CISN and (b) coumarin-induced venous limb gangrene. CISN most often affects the breast, abdomen, thigh, buttock, and calf and often is symmetrical; it is usually associated with congenital or acquired abnormalities in the protein C natural anticoagulant pathway. In contrast, venous limb gangrene occurs in patients with DIC associated with immune HIT or adenocarcinoma. This syndrome is characterized by microvascular thrombosis in a limb affected by DVT that leads to acral ischemic necrosis. (Reprinted with modifications from Warkentin TE. Heparin-induced thrombocytopenia: IgG-mediated platelet activation, platelet microparticle generation, and altered procoagulant/anticoagulant balance in the pathogenesis of thrombosis and venous limb gangrene complicating heparin-induced thrombocytopenia. Transfus Med Rev 1996;10:249-258, with permission.)
FIGURE 109.2 Coumarin-induced skin necrosis. Breast necrosis necessitating bilateral mastectomies occurred during the use of warfarin to treat pulmonary embolism complicating HIT. Follow-up studies showed no congenital deficiency in protein C, protein S, or antithrombin. Factor VLeiden and the prothrombin G→A20210 variant were not present. (Reprinted from Warkentin TE, Sikov WM, Lillicrap DP. Multicentric warfarin-induced skin necrosis complicating heparin-induced thrombocytopenia. Am J Hematol 1999;62:44-48, with permission.)
Often, multiple risk factors can be identified in individual patients (see Table 109.2).5, 6, 7, 8, 9, 10, 31, 32, 33, 34, 40, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76 An example is the concurrence of postpartum DVT, antiphospholipid syndrome, “loading doses” of warfarin, and premature discontinuation of heparin in one patient50; another is the concurrence of pulmonary embolism, factor VLeiden, “loading doses” of warfarin, and premature discontinuation of heparin in another.46
Abnormalities of the protein C natural anticoagulant pathway are a relatively common finding in patients with CISN. Indeed, congenital deficiency of protein C was the first hemostatic abnormality identified in some patients with CISN (although reports do not always distinguish hereditary deficiency from the reversible reduction expected in a patient receiving coumarin).68, 69, 70 Congenital deficiency of protein S45, 48, 49, 51, 52, 64, 71 and of antithrombin74 also has been observed, as has been the presence of factor VLeiden,46, 49, 53, 63, 72, 73 a common mutation that renders factor V less susceptible to proteolytic degradation by activated protein C. Most patients with CISN have acute DVT (rather than a nonthrombotic indication such as atrial fibrillation)55 as their indication for oral anticoagulants,3 suggesting that associated clinical factors (perhaps thrombin generation related to an acute thrombus) are relevant in CISN pathogenesis.
Only gold members can continue reading. Log In or Register to continue

 The Field of Hemostasis and Thrombosis: Selected Translational Achievements
The Field of Hemostasis and Thrombosis: Selected Translational Achievements
 Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
Structure and Function of Vitamin K-Dependent Coagulant and Anticoagulant Proteins
 Integrín αIIbβ3 and Platelet Aggregation
Integrín αIIbβ3 and Platelet Aggregation
 Inherited Thrombocytopenias
Inherited Thrombocytopenias
 Unusual Sites of Arterial Occlusion
Unusual Sites of Arterial Occlusion
 Blood Management in the Cardiovascular Surgical Patient
Blood Management in the Cardiovascular Surgical Patient



