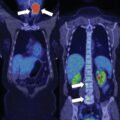
When a patient presents with an acute onset of severe Cushing syndrome (CS) due to metastatic adrenocortical carcinoma (ACC), clinicians ask: “Should the primary tumor be resected?” This is a good question, and many times the best answer is uncertain. However, in general, if the primary ACC can be resected without too much operative-related morbidity, it makes sense to debulk the “cortisol-secreting factory.” In this way, it provides the patient with a better quality of life while giving clinicians an opportunity to initiate treatment trials for the residual metastatic ACC.
Case Report
The patient was a 46-year-old woman who until recently had been quite healthy. Her only medication was losartan 50 mg daily for chronic hypertension. Two months previously she started developing signs and symptoms of CS, which included 30-pound weight gain; facial fullness; supraclavicular fat pads ( Fig. 27.1 ); abrupt onset of acne affecting the face, neck, chest, and back; proximal muscle weakness; fatigue; accelerated hypertension; and ankle edema. On physical examination her body mass index was 42 kg/m 2 and blood pressure 150/104 mmHg. She was overtly cushingoid with a full, round, plethoric face. She had marked acne of the face, neck, upper back, and upper chest. There was hirsutism involving the chin, sideburn areas, and upper lip. She had marked supraclavicular fat pads. There were no purple-red abdominal striae. She had 1+ ankle edema bilaterally.

INVESTIGATIONS
The baseline laboratory test results are shown in Table 27.1 . Marked corticotropin (ACTH)-independent CS was clearly documented. In addition to cortisol, her adrenal tumor was hypersecreting adrenal androgens. There was associated hypokalemia and hyperglycemia.
| Biochemical Test | Result | Reference Range |
| Sodium, mmol/L | 143 | 135–145 |
| Potassium, mmol/L | 2.3 | 3.6–5.2 |
| Fasting plasma glucose, mg/dL | 231 | 70–100 |
| Creatinine, mg/dL | 0.9 | 0.6–1.1 |
| 8 am serum cortisol, mcg/dL | 57 | 7–25 |
| 4 pm serum cortisol, mcg/dL | 51 | 2–14 |
| ACTH, pg/mL | <5 | 10–60 |
| Aldosterone, ng/dL | <4 | ≤21 |
| Plasma renin activity, ng/mL per hour | <0.6 | ≤0.6–3 |
| DHEA-S, mcg/dL | 767 | 18–244 |
| Total testosterone, ng/dL | 152 | 8–60 |
| 24-Hour urine cortisol, mcg | 462 | 3–45 |
Related posts:
 45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
45-Year-Old Woman With Corticotropin-Independent Cushing Syndrome and Bilateral Adrenal Adenomas
 Adrenocortical Carcinoma Associated With Multiple Endocrine Neoplasia Type 1
Adrenocortical Carcinoma Associated With Multiple Endocrine Neoplasia Type 1
 Cryoablation Therapy for Metastatic Paraganglioma
Cryoablation Therapy for Metastatic Paraganglioma
 Cushing Syndrome in the Setting of Multiple Endocrine Neoplasia Type 1
Cushing Syndrome in the Setting of Multiple Endocrine Neoplasia Type 1
 A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
A Huge Adrenal Myelolipoma in a Patient With a Suboptimally Controlled Congenital Adrenal Hyperplasia
 Catecholamine-Secreting Paraganglioma in Pregnancy
Catecholamine-Secreting Paraganglioma in Pregnancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


