CORTICOTROPIN-INDEPENDENT CUSHING SYNDROME
Part of “CHAPTER 75 – CUSHING SYNDROME“
Primary nodular hyperplasia, adrenocortical adenomas, and carcinomas as well as rare cases of ectopic cortisol production by tumor are found in 30% of patients presenting with Cushing syndrome.25
PRIMARY BILATERAL MICRONODULAR HYPERPLASIA
Primary bilateral micronodular hyperplasia is characterized by the presence in the adrenal cortex of one or more yellow nodules visible to the naked eye and 2 to 3 cm in diameter. Its pathogenesis is unknown. Whether this type of hyperplasia is of primary adrenal origin or the result of a combined mechanism by which the pituitary predominates initially but the adrenal eventually becomes autonomous, is not clear.26 Increased adrenocortical cell sensitivity to ACTH has also been suggested.27
Histologically, the micronodules consist of clear cells arranged in acini and cords, and are occasionally encapsulated and surrounded by simple or micronodular cortical hyperplasia. The frequency of mitotic figures is low. In one form of ACTH-independent micronodular adrenal disease, darkly pigmented micronodules are seen in the presence of atrophy of the perinodular adrenal tissue, disorganization of normal zonation of the cortex, and small glands28 (Fig. 75-3). Microscopically, the nodules are
composed predominantly of large globular cortical cells with granular eosinophilic cytoplasm that often contains lipofuscin.
composed predominantly of large globular cortical cells with granular eosinophilic cytoplasm that often contains lipofuscin.
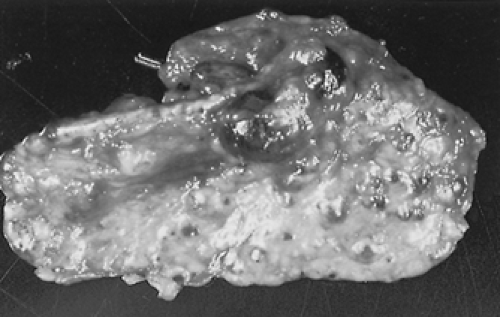 FIGURE 75-3. Appearance of an adrenal gland with pigmented micronodular hyperplasia removed from a patient with familial, corticotropin-independent Cushing syndrome. The patient was also found to have an atrial myxoma and a Sertoli cell testicular tumor.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|


