Clinical Manifestations and Diagnosis of Venous Thromboembolism
Clinical Manifestations and Diagnosis of Venous Thromboembolism
Henri Bounameaux
Arnaud Perrier
Pulmonary embolism (PE), the source of which is predominantly located in a thrombosis of the deep veins of the legs, is a major health concern. It is the third cause of mortality by cardiovascular disease after coronary artery disease and stroke. In Western countries, it remains a leading cause of death in the puerperium and the postoperative period. In addition, late consequences of deep vein thrombosis (DVT) may produce disabling leg symptoms including venous ulcers in a substantial proportion of patients, resulting in a considerable economic burden. Also, chronic pulmonary hypertension can develop in a small percentage of patients with PE within a few years and require pulmonary thrombendarterectomy, a difficult procedure performed in few dedicated surgical centers.
During the past two decades, the approach to diagnosing DVT and PE has changed in several major ways. First, it has been recognized that these two conditions are manifestations of a single entity, venous thromboembolism (VTE). Second, novel noninvasive diagnostic tools such as D-dimer (DD) measurement, venous compression ultrasonography (CUS), and multidetector computed tomography angiography (MDCTA) have become available. These tools have drastically reduced the need for invasive procedures such as phlebography and pulmonary angiography. Third, the clinical index of suspicion has progressively become lower, so the vast majority (80% or even more) of patients with suspected VTE do not have the disease. Fourth, efficient, mainly noninvasive strategies have been validated in large-scale outcome studies, and more attention has been paid to their cost implications.1,2
Finally, the appropriate approach to the diagnosis of VTE differs depending on the nature of the clinical setting: clinical suspicion of a first episode of DVT or PE, clinical suspicion of a recurrent episode of DVT or PE, or screening of asymptomatic DVT or PE in high-risk patients or in patients participating in clinical trials on prophylaxis or therapy of VTE.
CLINICAL MANIFESTATIONS
Clinical Classification of DVT and PE
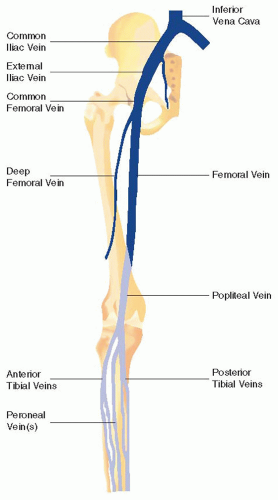
DVT is defined as the presence of a thrombus in the deep vein system. Although it may occur in all veins (lower and upper limbs, renal, mesenteric, splenic, portal or cerebral veins), it mainly affects the deep veins of the lower limbs (FIGURE 83.1). It must be distinguished from superficial thrombophlebitis, a more benign condition3 that usually does not require therapeutic anticoagulant therapy, except in selected patients.4 In general, deep vein thrombi arise in the calf veins (peroneal and posterior tibial veins, almost never anterior tibial veins) and may progress proximally, the so-called ascending thrombosis. In some cases (pregnancy, Cockett or May-Thurner syndrome, tumor), DVT may develop proximally, for example, in the common or external iliac vein, and progress distally, the so-called descending thrombosis.
Lower limb DVT may be proximal (from and including the popliteal vein and upward) or distal (in the calf below the popliteal veins), an important distinction because the embolic potential of proximal vein thrombosis is definitely higher than that of distal vein thrombosis.5 Calf muscle vein thrombi are considered as distal vein thrombosis though their clinical relevance is not well established.
DVT can be symptomatic or asymptomatic. Asymptomatic thromboses occur more frequently in bedridden patients, especially in the postoperative period, because symptoms (mainly pain and swelling) that are essentially due to venous stasis are usually more prominent in the upright position and thus in outpatients. Symptoms do not necessarily parallel clinical relevance: an asymptomatic iliac thrombosis in a bedridden patient carries a higher risk than a painful calf muscle vein thrombosis in an ambulant individual.
PE is defined as the presence of clots in the pulmonary arteries. The origin is from the lower limb deep veins in more than 90% of cases. Other sites of DVT can also result in PE, but this a rarer occurrence mainly because DVT is most often located in the lower limbs. Traditionally, PE was classified as massive or nonmassive but this classification is ambiguous because it is used alternatively to designate extensive PE on imaging (usually more than 50% amputation of the pulmonary vasculature), a finding only loosely correlated to clinical outcome, and PE accompanied by shock or at least systemic hypotension, which carries a high mortality and indicates thrombolytic treatment. Moreover, this classification does not account for those patients who have no systemic hypotension but present with right ventricular (RV) dysfunction secondary to PE, demonstrated on echocardiography. According to the ESC definitions, PE is now classified into the following categories (Table 83.1):6
High-risk (previously massive) PE: PE provoking shock or cardiorespiratory arrest (5% of cases)
Intermediate-risk (previously submassive) PE: PE provoking RV strain despite normal systemic blood pressure (30% of cases)
Low-risk (previously nonmassive) PE: PE associated with normal systemic blood pressure and normal RV function (65% of cases).
Presentation of Deep Vein Thrombosis
Classic symptoms of DVT include swelling and pain in the involved limb, but those symptoms are neither specific nor sensitive.7,8 Many nonthrombotic conditions can produce symptoms similar to those encountered in DVT, such as muscle strain, direct twisting injury to the leg and hematoma, Baker popliteal cyst, cellulitis, and the postthrombotic syndrome. The presence of one or several traditional risk factors (history of immobilization or prolonged hospitalization/bed rest, recent surgery, prior episode of DVT or PE, cancer, trauma, hormonal treatment, pregnancy or postpartum) increases the probability that symptoms are due to DVT. The most informative findings on clinical examination are pain on palpation of the deep veins, significant unilateral edema or swelling, and superficial venous dilation. Warmth, tenderness, and erythema are inconstant and less useful. It is nevertheless possible to assess the clinical probability of DVT in two or three categories based on a limited number of risk factors and clinical signs (see further Section).9 There is no correlation between clinical presentation and severity, as many thrombi are nonobstructive and are not associated with venous stasis or significant inflammation of the vessel wall or perivascular tissue. Severe forms of proximal vein thrombosis include the phlegmasia alba dolens that implies total occlusion of the deep venous system. The leg, then, must rely on the superficial venous system for drainage, which is not effective enough and results in edema, pain, and a white appearance of the leg. The next step in the disease progression is occlusion of the superficial venous system, thereby preventing all venous outflow from the extremity. At this stage it is called phlegmasia cerulea dolens. The leg becomes more swollen, cyanotic, and increasingly more painful. Additionally, the edema and loss of venous outflow leads to microcirculatory damage due to the very high venous pressure. Venous gangrene is the ultimate consequence. Phlegmasia cerulea dolens is frequently associated with cancer.
FIGURE 83.1 Anatomy of the deep veins of the lower limb. Note that the femoral vein was previously named “superficial femoral vein,” a potentially dangerous misnomer because this vein belongs to the deep vein system.
Presentation of Pulmonary Embolism
Clinical diagnosis of PE is not possible, due to the lack of sensitivity and specificity of clinical signs and symptoms.10 Incidental finding of PE is increasingly frequent (2.6% of patients undergoing a CT in a recent meta-analysis11), particularly in hospitalized patients or in cancer patients. However, PE is most often symptomatic and usually presents as one of the following three clinical pictures: pleuritic pain associated or not with dyspnea (65% of cases), isolated dyspnea, usually acute but sometimes slowly progressive (20%), or syncope (<10%). These clinical presentations correspond to three syndromes of different pathology and variable severity:12 (a) pulmonary infarction, (b) isolated dyspnea, and (c) shock, which defines high-risk PE (see next section).
Pleuritic pain is usually due to irritation of the visceral pleura by peripheral emboli. Hemoptysis may also be present, although more rarely. Although this syndrome is usually coined as “pulmonary infarction,” the histopathologic correlate is in fact an alveolar hemorrhage probably provoked by the efflux of blood from the high-pressure bronchial circulation in the segment obstructed by the embolus.13 The classic radiologic picture is a wedge-shaped pleural-based infiltrate that affects around 20% of patients.14 Other common chest x-ray anomalies include plate-like atelectasis and pleural effusion. Tachycardia and dyspnea are less frequent in this clinical syndrome reflecting the peripheral character and lesser hemodynamic repercussions of such pulmonary emboli.12
In the isolated dyspnea syndrome, the absence of pleuritic pain is probably due to more proximal embolization of the pulmonary vasculature. Patients may complain of retrosternal chest pain oppressive in character evoking the differential diagnosis of angina. In fact, such pain probably reflects true myocardial ischemia due to increased RV wall tension and reduced right coronary artery flow. Tachycardia, although more frequent, is still present in only 45% of patients.12 The electrocardiogram is rarely normal, but its anomalies are often nonspecific. Although dyspnea is usually of abrupt or rapid onset, in some patients it may progress over several days.
Systemic arterial hypotension and shock are the hallmark of high-risk PE causing acute severe pulmonary hypertension and RV failure. It is usually due to large central clots. Although suggestive of PE in patients with obvious risk factors such as recent surgery, syncope may be a misleading presentation.15 Suspected high-risk PE with shock is a distinct situation requiring a specific diagnostic approach detailed in Section 5.2.2.
Table 83.1 Risk stratification of patients with PE
Adapted from Torbicki A, Perrier A, Konstantinides S, et al. Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J 2008;29:2276-2315.
DIAGNOSTIC TOOLS
Diagnostic Criterion Standards for DVT and PE
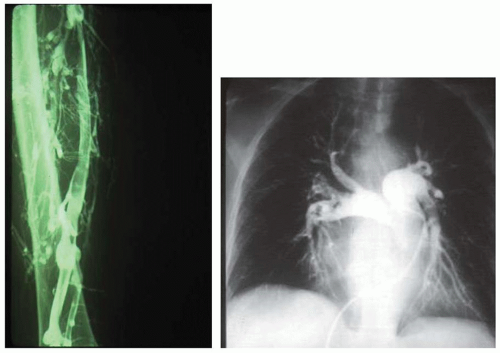
Ascending phlebography is still considered the diagnostic standard for diagnosing DVT but it is invasive, costly, and not devoid of risk. It consists of injection of iodinated contrast dye in a superficial foot vein with sequential radiograms of the leg to follow the dynamic course of the contrast in the veins. Tourniquets can be used to force the dye into the deep veins but their use is controversial. The documentation is adequate when images are obtained in different views, and a filling defect surrounded by contrast is characteristic for a fresh thrombus (FIGURE 83.2, left). It is still used as the standard surrogate endpoint in thromboprophylactic trials for efficacy assessment of new drugs after orthopedic surgery. It can be used for quantification of the thrombotic burden, for example, by Marder score.16 In clinically suspected individuals, however, it has been largely replaced by CUS. In a classic series by Hull et al.17 of 160 patients clinically suspected of DVT and left untreated based on a normal phlebogram, the 3-month thromboembolic risk was 1.9% (95% confidence interval [CI] 0.4% to 5.4%), indicating the potential of even the gold standard for false negatives. That figure is the benchmark for comparing the safety of other diagnostic tests to rule out DVT.
Although it is considered the criterion standard for diagnosing PE, pulmonary angiography is difficult to interpret, frequent disagreement occurring even between expert readers,18 more often on the absence (17% of angiograms) than on the presence of PE (8% of angiograms).19 The 3-month thromboembolic risk in patients left untreated after an angiogram that was considered normal was 1.7% (95% CI 1.0 to 2.7) in a systematic review pooling the results of eight series totaling 1,050 patients.20 The test is also costly, invasive, and not devoid of hazards. Moreover, the mortality due to pulmonary angiography was 0.2% (95% CI 0 to 0.3) in a pooled analysis of five series with a total of 5,696 patients.21 However, the rare deaths attributable to pulmonary angiography occurred in very sick patients with hemodynamic compromise or acute respiratory failure. Nevertheless, pulmonary angiography provides excellent anatomic views of the arterial vasculature of the lungs (FIGURE 83.2, right) and allows quantification of the embolic burden quite precisely, for example, by the Miller et al.22 index. Because of its invasive character, it should probably be restricted to patients for whom a clinically likely diagnosis could not be confirmed by other means or in those patients for whom endovascular treatment of PE is being considered.
In fact, phlebography and angiography are no longer used routinely in patients with a clinical suspicion of DVT or PE. Nevertheless, they still have a role in patients in whom the clinical likelihood of an acute thromboembolic event is high and in whom noninvasive tests have remained negative or inconclusive. Although valid, that change in clinical practice will probably result in decreasing expertise among radiologists performing these exams, which may decrease their accuracy in the future and further restrict their roles for routine use. Contemporary diagnostic standard equivalents are diagnostic criteria that have been proven safe in outcome studies with clinical 3-month follow-up. Admittedly, this standard is appropriate to ensure that a rule-out criterion has a high negative predictive value and safety, but does not inform on specificity and positive predictive value since positive tests in modern diagnostic strategies are no longer verified by the gold standard.
Obsolete Tests
While venous occlusion plethysmography and continuous wave Doppler flow examination are only used in anecdotal situations nowadays, electrocardiogram, arterial blood gases, and chest x-ray are still part of the so-called prior clinical probability assessment in patients with suspected PE although they no longer belong to the diagnostic tools. The same applies to the125I Fibrinogen uptake test in the lower legs in suspected DVT. This method has been utilized mainly for screening in clinical studies of thromboprophylactic regimens in the 70s and 80s.
FIGURE 83.2 The historical diagnostic gold standards for DVT (phlebography, left) and PE (pulmonary angiography, right). The arrows point to filling defects surrounded by contrast dye (characteristic for a fresh thrombus) in the femoral vein (left), in the inferior lobar artery left, and in all lobar arteries right (right).
Clinical Probability Assessment
Sensitivity and specificity of clinical symptoms and signs, and abnormalities of blood gases, chest radiograph, and electrocardiogram in suspected DVT or PE are low when considered singly. The electrocardiogram is usually normal in small peripheral PE. Larger PE may induce modifications such as large P waves in leads II, III, and AVF, the S1Q3T3 pattern, or ST segment depression in leads V1 to V4. A right bundle branch block or right axis deviation is also possible.23 Hypocapnia and hypoxemia are frequent in PE. However, approximately 20% of patients with proven PE have a normal arterial oxygen pressure and alveoloarterial oxygen gradient.24 The most frequent anomalies of the chest radiograph are cardiomegaly, pleural effusion, plate-like atelectasis, and elevated hemidiaphragm.14 Pulmonary artery enlargement and oligemia are rare and nonspecific. The typical infiltrate of so-called pulmonary infarction has already been discussed. Nevertheless, the chest radiograph remains extremely useful in a patient with suspected PE for differential diagnosis with conditions such as left ventricular failure, pneumonia, or pneumothorax.
Clinicians can combine these findings and other signs or symptoms very effectively either implicitly or by prediction rules in order to classify patients according to their probability of having the disease, the so-called prior clinical probability. As a practical tool for assessing prior clinical probability in suspected DVT, the Wells score25 and its simplified version26 have gained wide acceptance in spite of its partial subjectivity (Table 83.2). It is probably not more accurate than the simple implicit evaluation. However, it is easier to teach to junior physicians and allows discussing occasional disagreements among experienced clinicians on explicit grounds. Moreover, it has been shown that interobserver reliability was higher when using an explicit clinical model (kappa coefficient of agreement = 0.62 vs. 0.33 for implicit evaluation).27 Nevertheless, both the implicit assessment and the explicit Wells score allow categorizing usefully patients in low, intermediate, or high clinical probability groups in which the prevalence of DVT is approximately 5%, 20%, and 80%, respectively.
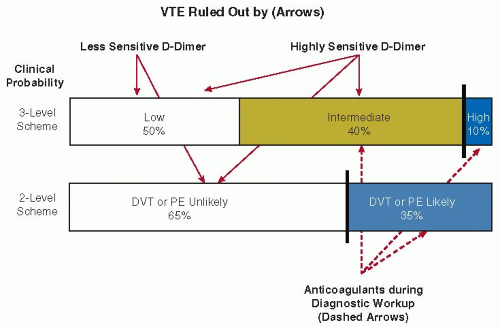
Likewise, the initial step of any diagnostic workup in suspected PE consists of assessing the clinical probability of the patient having the disease. The aim of this step is to (a) identify the patients (probably those with a high or intermediate clinical probability) who require anticoagulant treatment while awaiting the results of diagnostic tests and (b) select the patients (those with a non-high clinical probability) in whom the diagnosis of PE can be excluded on the basis of a negative DD test result, also in relation with the type of DD assay (see also below) (FIGURE 83.3).
Two scores have been widely used (Table 83.3).28,29 All these means of assessing clinical likelihood of PE allow a fairly accurate classification of patients into three categories corresponding to a prevalence of the disease of 5% to 10% (low clinical probability), 20% to 30% (intermediate clinical probability), and 60% to 80% (high clinical probability). Most patients with suspected PE have a low or intermediate clinical probability of having the disease. Those with a low or intermediate probability of PE can usually be investigated by entirely noninvasive algorithms. However, these rules also have limitations. The original Geneva score30 required arterial blood gas values while breathing room air, a variable that was not available in 15% of the patients in the external validation sample. The Canadian score (Table 83.3) includes the clinician’s judgment of whether an alternative diagnosis is more likely than that of PE.29 This criterion has major weight in this score and can clearly not be standardized, thereby hampering its use by nonclinical health professionals.
Table 83.2 Description of the Wells scores9,26 for patients with clinically suspected DVT
Items, Original Score
Points
Items, Simplified Score
Cancer
+1
Idem
+1
Paralysis or recent immobilization
+1
Idem
+1
Bedridden >3 d, or surgery/trauma <4 wk
+1
Idem
+1
Pain on palpation of the deep veins
+1
Idem
+1
Entire leg swollen
+1
Idem
+1
Calf swelling
+1
Idem
+1
Pitting edema (symptomatic side only)
+1
Idem
+1
Dilated superficial veins (symptomatic side only)
+1
Idem
+1
Previously documented DVT
+1
Alternative diagnosis at least as likely as DVT
-2
Idem
-2
Clinical Probability
Clinical Probability
Low
0
Unlikely
0-1
Intermediate
1-2
Likely
≥2
High
≥3
FIGURE 83.3 The objectives of clinical probability assessment. Clinical probability assessment can be expressed by means of 3-level or 2-level categories. It allows to rule out VTE by means of a negative DD test in patients with a low or unlikely assessment (less sensitive DD assays) or low and intermediate or unlikely assessment (highly sensitive DD assays). It also identifies patients who require anticoagulant treatment while awaiting results of diagnostic tests (patients with intermediate or high or likely assessment). The figures in the boxes represent the proportion of patients in the respective category.
The more recent “revised” Geneva score is entirely based on readily available clinical variables and is independent of physicians’implicit judgment (Table 83.3).28
In two recent outcome studies, the Wells score for PE has been used with a single cutoff of 4 points instead of two cutoffs.31,32 This resulted in a classification of patients into two clinical probability categories (PE unlikely or likely) instead of the traditional three levels of probability (low, intermediate or high), which would theoretically allow the use of a less sensitive DD assay in a higher proportion of patients than when using the three-level probability scheme but is further from implicit clinical judgment. Further simplifications of both the Wells rule and the revised Geneva score, in which all items carry the same weight, have also been proposed and have undergone external validation.33,34
In a systematic review and meta-analysis of the performance of all available clinical prediction rules for suspected PE,35 it was concluded that the various prediction rules have a similar accuracy in suspected PE. However, they are not identical and the choice between the various prediction rules and classification schemes must be guided by the local prevalence of PE, the type of patients considered (outpatients or inpatients) and the type of DD assay used. When using a highly sensitive DD assay, a three-level classification scheme is preferred because it mimics more closely clinicians’ empirical reasoning and potentially rules out VTE in a higher proportion of patients. Less-sensitive DD assays should be used in combination with the Wells score with two levels of probability (VTE likely or unlikely) as these assays are not able to exclude VTE in 40% of the patients in the intermediate clinical probability category, and the VTE unlikely category includes a higher proportion of patients than the low probability class. The performance of the Wells score for PE is sensitive to the overall prevalence of PE in the population of patients with suspected disease: in a series in which the prevalence of PE was higher than 20%, the prevalence of PE in the low and intermediate probability categories was significantly higher (16%, pooled average) than in series with a lower prevalence of the disease (3.4%). This is not a problem when using a highly sensitive DD assay, but might be with less-sensitive assays. We therefore advise using the revised Geneva score in populations with a prevalence of PE above 20% as that rule has been derived and validated in such settings. Finally, the Wells score for PE (two—or three-level) is the only validated score in inpatients.
Table 83.3 Description of the two most widely used scores for clinical probability assessment in patients with clinically suspected PE
Surgery (under general anesthesia) or fracture (of the lower limbs) within 1 mo
+2
Recent surgery or immobilization
+1.5
Active malignancy (solid or hematologic malignancy, currently active or considered as cured since <1 y)
+2
Clinical signs of DVT
+3
Unilateral lower limb pain
+3
Alternative diagnosis less likely than PE
+3
Hemoptysis
+2
Hemoptysis
+1
Heart rate 75-94 bpm
+3
Cancer
+1
Heart rate ≥95 bpm
+5
Pain on lower limb deep vein palpation and unilateral edema
+4
Clinical Probability
Clinical Probability
Low
0-3
Initial rule
Intermediate
4-10
Low
0-1
High
≥11
Intermediate
2-6
High
≥7
Dichotomized rule
Unlikely
≤4
Likely
>4
Fibrin D-Dimer Measurement
DD is a degradation product of cross-linked fibrin and its blood concentration is increased in patients with acute VTE. It has been used as an adjunct in the diagnostic workup of DVT and PE for 20 years.36 When assayed using a quantitative enzyme-linked immunosorbent assay (ELISA) or an automated turbidimetric assay, the DD level has been shown to be highly sensitive (more than 95%) in acute DVT or PE, usually with a cutoff value of 500 µg/L. Hence, a DD level below this value reasonably excludes acute VTE, at least in patients with a low or intermediate clinical probability. Their 3-month thromboembolic risk is <1%, as shown in a meta-analysis on the use of the highly sensitive VIDAS d-dimer Exclusion test.37 According to these data, PE could be ruled out in about one third of clinically suspected outpatients. This proportion, however, varies according to patient categories (Table 83.4).38,39,40,41,42,43,44,45,46,47 The Tinaquant test, an immunoturbimetric assay, has also been largely validated.32 The result was negative ruling out PE in 41% of patients who had either a low clinical probability of PE or were classified as “PE unlikely” according to the dichotomized Wells rule. The 3-month thromboembolic risk was also <1%. Finally, the SimpliRed assay, a whole blood less-sensitive bedside test has also been well validated45 but interobserver variability may be a problem, and exclusion of the disease is only possible in patients with low or “unlikely” clinical probability. Conversely, patients with a high clinical probability should not be tested for DD because a concentration below the diagnostic cutoff is rare in this category of patients,39 and above all because the upper limit of the 95% CI for the 3-month occurrence of PE remains above 3% despite a negative result.
Table 83.4 Diagnostic yield of DD for ruling out PE in specific patient populations
The number needed to test (NNT) reflects the number of patients in whom DD measurement has to be performed to rule out one PE.
a No patient with negative DD result in this cohort
In order to increase the exclusion rate of DD in elderly patients, a European group devised an age-dependent DD exclusion cutoff for PE that was based on 5,132 patients aged 50 or above from four previous prospective cohort studies.48 The individualized DD cutoff value was defined as patient’s age × 10 µg/L in patients aged above 50. In 1,331 patients in the derivation set with an “unlikely” score from clinical probability assessment, PE could be excluded in 42% with the new cutoff value versus 36% with the old cutoff value (<500 µg/L). In the two validation sets, the absolute increase in the proportion of patients with a DD below the new cutoff value compared with the old value was 5% and 6%, respectively. This increase was largest among patients aged above 70 years, ranging from 13% to 16% in the three datasets. The failure rates (all ages) were 0.2% (95% CI, 0 to 1.0) in the derivation set and 0.6% (95% CI, 0.3 to 1.3) and 0.3% (95% CI, 0.1 to 1.1) in the two validation sets, respectively. Thus, it appears that an age-adjusted DD cutoff point, combined with clinical probability, greatly increases the proportion of older patients in whom PE could be safely excluded; this is presently being externally further validated in a prospective clinical outcome study. It is clear that this rule will be valid only for the two tests that were used in the original studies, the VIDAS and the Tinaquant DD tests. A similar approach has been proposed for pregnant women clinically suspected of DVT49 but the proposed increased cutoffs clearly require validation in prospective management studies.
Although DD is very specific for fibrin, the specificity of fibrin for VTE is poor. Indeed, fibrin is produced in a wide variety of conditions such as cancer, inflammation, infection, and necrosis. Hence, a DD concentration above 500 µg/L (the diagnostic cutoff for many assays) has a poor positive predictive value for VTE, and cannot reliably rule in the disease. Nevertheless, based on the results of a retrospective analysis of a large patient sample, Bosson et al.50 suggested that a DD level above 2,000 µg/L was predictive of the presence of PE, independently of the clinical score with an odds ratio of 6.9. They noted, however, that this result requires clinical validation in a prospective study, particularly because the PE prevalence in their series was high: 27%, 58%, and 85% in the low, intermediate and high clinical probability categories, respectively. The Geneva group had previously reported that patients with an intermediate or high clinical suspicion of PE and a DD level above 4,000 µg/L had a positive likelihood ratio of five of having the disease, but few clinicians would accept the diagnosis just on this basis.51 Recent quantitative point-of-care (POC) tests have shown a promising sensitivity of 96% but only in patients suspected of DVT and in a relatively small sample size.52
Only gold members can continue reading. Log In or Register to continue
 The Field of Hemostasis and Thrombosis: Selected Translational Achievements
The Field of Hemostasis and Thrombosis: Selected Translational Achievements
 Integrín αIIbβ3 and Platelet Aggregation
Integrín αIIbβ3 and Platelet Aggregation
 Coagulation-Independent Signaling of the Extrinsic Coagulation Pathway
Coagulation-Independent Signaling of the Extrinsic Coagulation Pathway
 Inherited Thrombocytopenias
Inherited Thrombocytopenias
 Pathogenesis and Treatment of Biomaterial-Associated Thrombosis
Pathogenesis and Treatment of Biomaterial-Associated Thrombosis
 Blood Management in the Cardiovascular Surgical Patient
Blood Management in the Cardiovascular Surgical Patient



