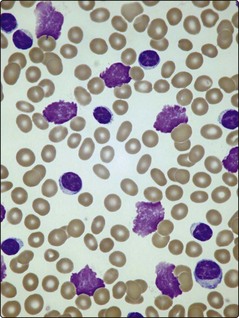
23 Where problems do arise, patients commonly complain of symptoms of anaemia, lymphadenopathy, unusually persistent or severe infections and weight loss. The most frequent findings on examination are lymphadenopathy and splenomegaly. In more advanced cases other tissues such as skin, the gastrointestinal tract, the central nervous system, lungs, kidneys and bone may be infiltrated by leukaemic cells. Occasionally there is transformation into a poorly differentiated large cell lymphoma which carries a poor prognosis (Richter syndrome). The immunodeficiency in CLL is caused mainly by hypogammaglobulinaemia, which predisposes to infections (Fig 23.1) and also accounts for an increased incidence of other malignancies. The diagnosis is suggested by a high lymphocyte count confirmed by the blood film appearance. Lymphocyte counts in CLL exceed 5 × 109/L and may reach levels of 500 × 109/L or more. The cells resemble normal mature lymphocytes but are often slightly larger with a tendency to burst during preparation of blood films, resulting in ‘smear cells’ (Fig 23.2). Unexplained persisting lymphocytosis in an elderly person should always suggest CLL. The diagnosis is made by proving that the lymphocytosis is a proliferation of clonal B-cells; this is most simply demonstrated by using in situ or flow cytometry techniques (see p. 21) to show that the cells have characteristic B-lymphocyte antigens and that a single immunoglobulin light chain (kappa or lambda) exists on the cell surface (i.e. it is a monoclonal population). The bone marrow aspirate shows increased numbers of small lymphocytes and a trephine biopsy is worthwhile as the pattern of lymphocyte infiltration gives prognostic information. The blood film appearance may suggest autoimmune haemolysis or autoimmune thrombocytopenia, both of which can complicate CLL.
Chronic lymphocytic leukaemia
Clinical features
Diagnosis
Chronic lymphocytic leukaemia