Breast-conserving therapy (BCT), a combination of breastconserving surgery (BCS) followed by whole breast irradiation, is an established standard of care for local-regional treatment for early-stage breast cancer. The first clinical trials investigating BCT began more than three decades ago. The outcome data from these trials, including a meta-analysis of all of the trials (1), provided clear evidence that breast-conserving surgery followed by whole breast radiation achieved long-term survival equivalent to mastectomy.
Currently, most patients with newly diagnosed breast cancer are candidates for BCT. The increased use of mammographic screening, and improved public education about breast cancer, have dramatically increased the percentage of cases that present with early-stage disease. Studies have demonstrated that BCT positively impacts patient well-being and quality of life. Over time, as experience has been gained with BCT and the use of adjuvant systemic therapy has become routine even for patients with stage 1 breast cancer, rates of local recurrence (LR) after BCT have declined to less than 0.5% per year (2). Despite the established efficacy and excellent outcomes of BCT, recent data show an increase in the utilization of therapeutic mastectomy and prophylactic contralateral mastectomy, particularly among younger patients (3).
This chapter will review the progress that has been made in BCT, including the current selection criteria for BCT, the importance of radiation therapy (RT) as a component of BCT, comparing the approaches of conventional whole breast irradiation versus accelerated whole breast irradiation versus accelerated partial breast irradiation, the patient-, treatment-, and tumor-related factors that influence outcome, and the technical details of optimizing both surgical and radiation treatment of early-stage breast cancer.
SELECTION CRITERIA FOR BREAST-CONSERVING THERAPY
BCT is generally reserved for patients with tumors smaller than 5 cm. However, more important than absolute tumor size is the relationship between tumor size and breast size. The tumor must be small enough, in relation to the size of the breast, to permit the tumor to be resected with clear margins and an acceptable cosmetic result. In patients with invasive breast cancer in which the tumor-to-breast size ratio is unfavorable, preoperative chemotherapy or endocrine therapy can be used to decrease the tumor size sufficiently to permit BCT (see Chapters 54 and 55).
The 2012 National Comprehensive Cancer Network (NCCN) guidelines to contraindications for BCT requiring RT include:
Absolute Contraindications
Prior RT to the breast or chest wall
Breast cancer early in a pregnancy that would necessitate RT during pregnancy
Widespread disease that cannot be incorporated by excision through a single incision that achieves negative margins with a satisfactory cosmetic result
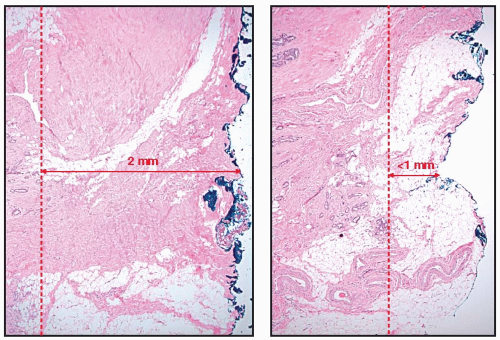
FIGURE 35-1Sampling error and margin assessment. On the left is an initial section with a margin width of 2 mm. A slightly deeper section, shown on the right, was taken for special studies and showed a margin width of less than 1 mm.
Relative Contraindications
Active connective tissue disease involving the skin (especially scleroderma and lupus, but not rheumatoid arthritis)
Focally positive margin in the absence of an extensive intraductal component (see below)
Women with a known or suspected genetic predisposition to breast cancer
The evaluation for BCT includes a history, physical exam, and diagnostic mammography. Using this approach, patients suitable for BCT can be identified with a high degree of success as illustrated by a population-based study of 800 women attempting BCT in which surgery was successful in 88%. Of the 12% who were converted to mastectomy, re-excision was attempted in only one-third, suggesting that the 88% is a minimum estimate (4). There is controversy regarding the role of additional imaging studies, particularly magnetic resonance imaging (MRI) of the breast, in selecting patients for BCT. A meta-analysis of 3,112 patients in 9 studies with comparison cohorts treated with and without MRI found no difference in the need for re-excision or unexpected conversion to mastectomy, after age adjustment, in patients managed with and without MRI (5). The lack of impact of MRI on LR rates is discussed in the following section in the context of margins.
MARGINS AND LOCAL RECURRENCE
Margin width is assessed by applying ink (ideally colored to reflect the individual margins) to the surface of the specimen. Margin width is the distance between tumor cells and inked surface. A negative margin is defined by “no ink on any cancer cells.” Despite the NCCN guidelines, what constitutes an adequate margin is controversial (6). In surveys, no single margin width is endorsed by more than 50% of respondents (7, 8). Many practitioners favor a margin of 2 mm or even greater. As a result, re-excision is commonly used, even with a negative margin. Part of this is due to difficulties in margin assessment. Specimen processing is not standardized and varies between institutions. Sampling error is another difficulty. Even with fastidious assessment of margins, however, only a very small percentage of the entire margin is assessed. This is illustrated in Figure 35-1. On the left is an initial section with a margin width of 2 mm. A slightly deeper section, shown on the right, was taken for special studies and showed a margin width of less than 1 mm. A meta-analysis of 21 studies reporting LR relative to margin width showed that LR was significantly greater with a positive margin than a negative margin, but increasing margin width did not significantly decrease LR (9).
It is becoming increasingly clear that factors other than margin width are the primary determinants of local control. In more recent studies, which include the routine use of adjuvant systemic therapy, substantially reduced rates of LR have been seen. This is illustrated in the 10-year rates of LR in successive National Surgical Adjuvant Breast and Bowel Project (NSABP) trials in node-negative patients treated with BCT (2). In NSABP B-13, which randomized patients with estrogen receptor (ER) negative cancer to adjuvant chemotherapy or not, 10-year LR was 15.3% without chemotherapy and only 2.6% in patients with chemotherapy. Similarly, in NSABP B-14, which randomized patients with ER positive cancer to adjuvant tamoxifen or placebo, 10-year LR was 11.0% with placebo and only 3.6% in patients treated with tamoxifen. During these trials, the NSABP used “no ink on tumor” as the definition of a negative margin. Studies examining the impact of adding trastuzumab to adjuvant chemotherapy in women with HER2-overexpressing tumors demonstrate an additional 40% reduction in the risk of LR, with a median follow-up of 1.5 to 2.0 years (10). In a retrospective study from Memorial Sloan-Kettering Cancer Center, 3-year rates of LR decreased from 7% to 1% in patients with HER2-overexpressing tumors after the addition of trastuzumab to chemotherapy (11). Updated results from Dana-Farber Cancer Institute/Brigham and Women’s Hospital, and Massachusetts General Hospital included 1,434 patients; 91% were treated with adjuvant systemic therapy (not including trastuzumab), and with a median follow-up time of 85 months, the 5-year rate of LR was 1.6% and the overall crude rate of LR was 3.1% (12). (These rates are expected to double at a median follow-up of 10 years.) In this study, as well as several others, the main prognostic factor for LR was biologic subtype approximated by hormonal receptors, HER2 status, and histologic grade, with Luminal A = HR+, HER2-, Gr 1-2; Luminal B = HR+, HER2-, Gr 3; Luminal-HER = HR+, HER2+; HER2 = HR-, HER2+; and triple negative = HR-, HER2-. The crude rate of LR by subtype was 1.5% for Luminal A, 4.0% for Luminal B, 1.0% for Luminal-HER, 10.9% for HER2+, and 8.8% for triple-negative cancers. Age was also in the final model, but the magnitude of the effect was much smaller, with a crude rate of LR of 6.5% for the patients in the lowest age quartile (ages 23 to 46) compared with only 0.9% for patients in the highest age quartile (ages 64 to 88). Margin status was not in the final model of prognostic factors for LR. These and other data indicate that the biological features of the tumor are most important in determining the risk of LR. Studies examining the relationship between molecular subtype, as approximated by receptor status, and LR are summarized in Table 35-1 (12, 13 and 14). Although definitions of the Luminal B subtype have varied over time, the lowest rates of LR are consistently seen in patients with Luminal A cancers and the highest rates in those with triplenegative cancers (12, 13 and 14), and this relationship persists even for T1a, b and microinvasive cancers (15) and in patients receiving neoadjuvant chemotherapy (16). The higher rates of LR in patients with triple-negative cancers have raised concern that these patients might benefit from treatment with mastectomy. However, patients with triple-negative cancers have the highest LR risk after both BCT and mastectomy, and retrospective studies do not demonstrate an improvement in local control after mastectomy compared to lumpectomy and radiation, even in this more aggressive tumor subset (17, 18 and 19). In multivariable analyses controlling for both conventional prognostic factors and biologic subtype, type of surgical procedure (mastectomy vs. BCT) is not a clinically significant predictor of LR for neither high-risk triple negative patients (18) nor the lower-risk ER positive subset (20).
There are additional lines of evidence that widely negative margins are not required (in the large majority of patients) for successful BCT when routine adjuvant systemic therapy is employed. Multiple studies have demonstrated that breast MRI in patients with a known primary identifies multifocal and multicentric cancers (located at a considerable distance from the known primary) in about 11% of patients (21) and triples the age-adjusted odds ratio of an initial mastectomy rather than BCT (5); however, the available studies do not demonstrate lower rate of LR with BCT in patients receiving MRI compared to those who have not (22, 23). Additional evidence for the concept that minimizing the subclinical tumor burden is not critical for reducing LR in the current era of multimodality treatment comes from the results of the American College of Surgeons Oncology Group (ACOSOG) Z0011 trial. In that study, women undergoing breast-conserving surgery, sentinel node biopsy, and whole breast irradiation, who had metastases in one or two sentinel lymph nodes, were randomized to axillary dissection or no further axillary treatment. All patients received adjuvant systemic therapy. In spite of the finding of additional nodal metastases in 27% of the axillary dissection group, only 0.9% of patients in the sentinel node-only group experienced a first recurrence in the axilla (24).
TABLE 35-1 Local Recurrence after Breast-Conserving Therapy and Molecular Subtype
In considering the use of margins in BCT, it is useful to note that breast cancers are very often multifocal, with at least 40% of cases having microscopic foci greater than 2 cm from the edge of the cancer. This frequency is not influenced by tumor size, and these microscopic foci are more often ductal carcinoma in situ (DCIS) than invasive cancer. A key concept in the practice of BCT is that margin evaluation (and mammography) are used to insure that there is only limited residual cancer capable of being eradicated with conventional doses of RT, but not to insure there is no cancer remaining.
Thus, the current evidence indicates that in the context of highly effective systemic therapy, no ink on tumor is a sufficient margin for the large majority of patients. However, there are some exceptions, and these include cancers with an extensive intraductal component (EIC), patients receiving preoperative chemotherapy, and pure DCIS. EIC is defined by prominent DCIS within the tumor (˜25%) and present in adjacent tissue. The presence of an EIC predicted for LR in patients treated with BCT without margin evaluation; however, EIC ceased to be a prognostic factor for LR with the routine use of margin evaluation. The presence of an EIC also predicts for patients with prominent residual disease after a gross excision of the tumor. Similar considerations exist for patients with pure DCIS, and this is supported by clinical data (25). In both situations, obtaining clearly negative margins is prudent. Finally, since tumors typically respond to preoperative chemotherapy in a honeycomb pattern rather than a concentric pattern, obtaining clearly negative margins is also prudent in the setting of preoperative chemotherapy.
ROLE OF RADIATION THERAPY IN BREAST-CONSERVING THERAPY
Radiation treatments play an important role in successful BCT for patients with invasive breast cancer. It has been clearly demonstrated that radiation treatment of the ipsilateral breast reduces the probability of LR after lumpectomy. More importantly, meta-analyses from the Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) of all the randomized prospective trials comparing BCS or mastectomy with or without postoperative RT indicate that by eradicating persistent local disease after surgery, RT use reduced the risk of subsequent death from breast cancer. The first analysis was published in 2005 and described a 4 to 1 ratio between avoiding LR at 5 years and improving survival at 15 years. After either BCS or mastectomy, RT proportionally reduced LR by 70%. An updated analysis was published in 2011 restricted to patients treated with BCS (26). In this updated analysis, 7 trials of BCS in low-risk patients, most treated with adjuvant hormonal therapy and randomized to breast RT or not, were added to the original 10 trials in the 2005 publication for a total of 10,801 women, 3,143 deaths, and a median woman-years at risk of 9.5. Importantly, the EBCTCG moved from assessing the effect of RT on LR to its effect on first failure (or first recurrence, either LR or distant metastasis). Although commonly employed in studies on the local treatment of breast cancer, actuarial calculation of time to LR is, strictly, not statistically valid. As shown in Figure 35-2, RT proportionally reduced the annual rate of any failure (LR or distant metastases) over the first 10 years by about half (relative risk [RR] = 0.52) and proportionally reduced the annual rate of breast cancer death by about one-sixth. The absolute benefit of RT was greater in patients with the greater risk of recurrence. In node-negative patients, the absolute benefit was strongly correlated with age (inversely), tumor grade and size, and ER status, with very small absolute benefit seen in some subgroups. The updated EBCTCG analysis still demonstrates that local treatment is linked to improved long-term survival; however, the new 4:1 ratio is between the reduction in first failure at 10 years (not the reduction in LR at 5 years) and the reduction in mortality at 15 years.
FIGURE 35-2 The data from the EBCTCG meta-analysis of trials investigating breast-conserving surgery with or without breast radiation. Effect of RT after BCS on 10-year risk of any (local-regional or distant) first recurrence and on 15-year risks of breast cancer death and death from any cause in 10,801 women (67% with pathologically node-negative disease) in 17 trials. (From Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet 2011;378:1707-16, with permission.)
Do All Patients Treated with Breast-Conserving Therapy Require Radiation?
The initial trials that demonstrated a clear benefit for radiation in BCT included populations that were heterogeneous with respect to risk factors associated with LR. Therefore, the second generation of clinical trials studying BCT investigated whether radiation could be safely omitted in favorable subgroups. Unfortunately, most of these studies were unsuccessful in positively answering the question. For example, a single-arm, 82-patient prospective trial conducted at Harvard Medical School investigated whether breast radiation could be omitted in patients with pT1N0 breast cancer without an extensive intraductal component or lymphovascular space invasion that was excised with 1 cm or greater margins. Despite these favorable features, the trial was closed early after the breast recurrence rate exceeded the predefined stopping rules. The LR rate after a median follow-up of 86 months was 23% (27). These recurrence rates were similar to those seen in a trial from the Milan Cancer Institute that randomized women with tumors 2.5 cm or smaller to a quadrantectomy and axillary dissection without radiation or this same surgery followed by breast irradiation. Despite a more extensive surgical procedure than what is routinely utilized in most North American trials, the 10-year risk of in-breast recurrence was markedly higher in the absence of RT (24%) compared with patients who received RT (6%) (p < .001) (28). Randomized trials from Sweden and Finland have also attempted to specifically address whether patients with stage I disease require RT after BCT, and in both of these studies, the use of radiation led to a highly significant improvement in local outcomes (29, 30). Finally, it is also clear from several trials that the use of adjuvant chemotherapy does not obviate the need for breast irradiation. For example, in the NSABP B-06 trial, chemotherapy was used for patients with lymph node-positive disease, and these patients had a 44% 20-year risk of in-breast recurrence without radiation compared to a rate of only 9% for those treated with lumpectomy, radiation, and chemotherapy (31).
The most recent randomized trials attempting to identify a favorable cohort with a low risk of in-breast recurrence without radiation have focused on postmenopausal women with hormone receptor positive stage I disease treated with breast-conserving surgery and hormonal therapy. The data from these trials are shown in Table 35-2 (32, 33, 34, 35, 36 and 37) and demonstrate that the combined modality treatment of breastconserving surgery, radiation, and adjuvant hormonal therapy is associated with a very low 5-year risk of in-breast or local-regional recurrence.
TABLE 35-2 Randomized Studies Comparing Radiation Use after Breast-Conserving Surgery in Patients with Stage I Disease Treated with Hormonal Therapy
LR, local recurrence; L-RR, local-regional recurrence; CALGB, Cancer and Leukemia Group-B.
In contrast, data from the Scottish trial and the NSABP B-21 trial suggest that the risk of in-breast recurrence remains clinically relevant with BCS and hormonal therapy alone. The one cohort of patients for whom BCS without radiation might be considered as an appropriate option are elderly females with an ER positive stage I breast cancer who are treated with hormonal therapy. The Cancer and Leukemia Group-B (CALGB) Intergroup trial randomized women 70 years of age and older with these disease characteristics to breast-conserving surgery plus tamoxifen or BCS, tamoxifen, and breast irradiation (35). With a median follow-up of 95 months, radiation reduced the localregional recurrence from 7% to 1% (36). It should be noted that approximately 1 of 6 of these patients enrolled in this study died of intercurrent disease by 5 years. Therefore, how these data should be applied to women over 70 years of age who have a longer life expectancy is less clear. To further study this question, investigators from Yale University reviewed the Surveillance, Epidemiology and End Results (SEER)-Medicare Database and identified 8,724 patients who met the eligibility criteria for this trial. They found similar 5-year outcome rates as those reported in the Intergroup trial (38). However, these investigators also were able to analyze patient subsets and found that the benefits of RT were of a clinically relevant magnitude for patients aged 70 to 79 who had no comorbidities. In contrast, those patients 80 years or older and those with multiple comorbidities had a higher risk of dying from non-breast-cancer-related causes within 5 years and therefore were not at high risk of developing an in-breast recurrence.
In conclusion, all of the clinical studies to date have indicated that without breast irradiation, the risk of LRs after breast-conserving surgery alone is too high and, therefore, breast irradiation should be considered a standard component of treatment for all women with early-stage invasive disease. This has become more feasible with the development of hypofractionated (shorter-course) approaches discussed later. Thus far, the attempts to define subsets of breast cancer patients with favorable early-stage disease that may not require RT by using standard clinical and pathologic criteria have been unsuccessful, with the possible exception of women over 70 years of age with stage I, ER positive disease who are willing to be treated with hormonal therapy. Studies are underway to find molecular markers that can reliably identify patients who may be adequately treated with breast-conserving surgery alone without the need for radiation.
Patient-Related, Disease-Related, and Treatment-Related Factors Associated with Local Outcome after Breast-Conserving Therapy
Patients treated with BCT have excellent rates of local control. The EBCTCG meta-analysis of the first generation of clinical trials investigating breast conservation reported a 5-year in-breast recurrence rate of 6.7% for patients with node-negative disease and 11% for those with node-positive disease (1). The respective 10-year in-breast recurrence rates for these cohorts were 10% and 13.1%, respectively. As previously indicated, there have been a number of changes that occurred over the past few decades that have favorably affected these rates. In part, these changes have come from a greater understanding of patient, disease, and treatment factors that are associated with LRs, and this has helped to refine the selection criteria for breast conservation and has led to changes in treatment techniques to improve outcomes.
Patient-Related Factors. An important patient-related factor that affects in-breast recurrence rates is patient age. Several single-institution studies have reported that young patient age, usually defined as age less than 30 to 40 years, is associated with an increased risk of local recurrence (LR), distant metastases (DM), and reduced disease-specific survival (39, 40, 41 and 42). This finding was also noted in an European Organisation for Research and Treatment of Cancer (EORTC) randomized trial that investigated the use of a tumor bed boost after whole breast irradiation. Overall, when patients from both arms of the study were evaluated, the 5-year inbreast recurrence rate for patients 40 years of age or less was 15%, compared to rates of 7% for patients aged 41 to 50 years, 4% for patients aged 51 to 60 years, and 3% for patients older than 60 years of age (39). Younger age has also been shown in some studies to adversely affect LR rates after mastectomy. A study from investigators at the University of Texas MD Anderson Cancer Center retrospectively evaluated the local-regional treatment outcome of 668 breast cancers in patients 35 years of age or less (40). In this series, patients with stage I disease who were treated with chemotherapy had acceptable local-regional treatment outcomes with either BCT or mastectomy. However, the patients with stage II disease treated with BCT (18%) or mastectomy without radiation (23%) had higher 10-year local-regional recurrence rates than those treated with mastectomy and postmastectomy radiation (6%). There is some evidence that the impact of young age on the risk of LR has decreased over time. In a population-based registry study, Van der Sangen et al. reported that the 5-year risk of LR in women less than 40 years of age undergoing BCT decreased from 11% for those treated from 1993 to 1998, to 3.8% for those treated between 2000 to 2005 (43). How much of the agerelated risk of LR is due to a higher proportion of unfavorable cancer subtypes, such as triple-negative disease, is unclear. Cancello et al. retrospectively examined patients enrolled in International Breast Cancer Study Group trials to determine the impact of age within breast cancer subtypes. In patients with Luminal A type tumors, no increase in LR was seen in those under 35 years of age compared to patients aged 35 to 50 years, but for other subtypes, there was a trend for very young age to be associated with an increased risk of LR, although this did not reach statistical significance in some groups due to sample size (44). As noted above in a recent series from the Dana-Farber Cancer Institute/Brigham and Women’s Hospital, and Massachusetts General Hospital in Boston, age was also in the final model along with subtype, but the magnitude of the effect was much smaller than for subtype, with a crude rate of LR of 6.5% for the patients in the lowest age quartile (ages 23 to 46) compared with only 0.9% for patients in the highest age quartile (ages 64 to 88). Additionally, both poor prognosis Amsterdam genetic signatures and high 21 gene recurrence scores (Oncotype Dx) are more frequent in younger women (45, 46); as a result, further research evaluating the interaction between molecular subtype and age is needed. At present, young age alone should not be considered a contraindication to BCT.
A second, important patient-related factor that can influence rates of LR is the presence of a germline mutation in BRCA1 or BRCA2. Investigators from Yale University determined BRCA gene status in 127 patients, 42 years of age or less, who were treated with lumpectomy and radiation, and found 22 with deleterious mutations. After 12 years, the rates of ipsilateral breast recurrence (49% vs. 21%; p = .007) and contralateral cancer (42% vs. 9%; p = .001) were both significantly higher in the patients with BRCA mutations (47). Many of these ipsilateral breast recurrences may actually be second breast cancers. Also, these high rates of in-breast recurrence may be significantly less in carriers who have undergone a bilateral oophorectomy. This finding was noted in a multicenter retrospective study that did not find an overall difference in the 10-year rate of in-breast recurrence in mutation carriers (12%) versus matched controls (9%). However, mutation carriers who had not had a bilateral oophorectomy experienced increased rates of in-breast recurrence compared to controls (hazard ratio [HR] 1.99; p = .04) (48). Age at initial cancer diagnosis also impacts the risk of subsequent cancers in the ipsilateral breast. Table 35-3 (47, 48, 49 and 50) displays published studies that have evaluated the rates of ipsilateral tumor recurrences and of contralateral breast cancer in BRCA mutation carriers. The choice of mastectomy versus BCT is influenced by patient preference, age, stage, and whether the mutation is in BRCA1 or BRCA2. Younger patients with early-stage breast cancer are encouraged to have mastectomy. Older patients can be considered for BCT, particularly if the breast cancer is more advanced and/or BRCA2 associated (see Chapter 17).
TABLE 35-3 Rates of Ipsilateral Tumor Recurrences and Development of Contralateral Breast Cancer in BRCA Carriers Treated with Breast-Conserving Therapy
Disease-Related Factors. One of the most important pathologic factors that affects rates of local control after BCT is surgical margins. When BCT was first introduced, the importance of achieving histologically negative margins was not recognized, and a number of patients in early BCT publications had either unknown margin status or positive surgical margins. Retrospective analyses indicated that such patients had higher rates of LR, particularly if the disease had an extensive intraductal component (defined as tumors that are predominantly non-invasive or tumors with a DCIS component comprising at least 25% and with DCIS present in surrounding normal breast tissue) (51). The fact that biologic factors are increasingly recognized as determinants of LR after both mastectomy and BCT has been discussed in detail, as has the role of systemic therapy in reducing LR and the lack of evidence that margins more widely clear than tumor not touching ink are necessary for the majority of breast cancer patients. The presence of ink on tumor remains an indication for re-excision, but when re-excision carries a significant aesthetic consequence, the degree of margin involvement should be considered. Specifically, some retrospective series have found that patients with a focally positive margin have better outcomes that those with margin involvement over a wider area. In one study, Vicini et al. (52) retrospectively reassessed margin status in 607 cases treated with BCT and reported a 12-year in-breast recurrence rate of 9% in patients with negative margins, 6% when a small amount of disease was close to the margin, 18% for those with an intermediate degree of disease close to the margin, 24% for those with a large volume of disease close to margin, and 30% for those with a positive margin. It is also useful to note that margins at the skin anteriorly or at the pectoral fascia posteriorly are not of concern since breast tissue does not extend beyond those margins. Good communication between the surgical and radiation oncologists is important in this regard.
Not surprisingly, the importance of margin status on LR is also affected by other factors, such as age, use of systemic therapy, and timing of radiation delivery. Park et al. (53) reported that the use of systemic treatments reduced the in-breast recurrence rates for patients with focally positive margins (8-year rate of 7%), whereas higher rates were seen in those with focally positive margins who did not receive systemic therapy and in all patients with more diffusely positive margins. Jobsen et al. (54) showed that margin status was of particular importance in women 40 years of age or less. In this younger cohort, the risk of in-breast recurrence according to margin status was 37% in those with positive margins compared with only 8% in those with negative margins. Finally, in a randomized prospective trial, investigators from Harvard Medical School found that patients with close or positive margins had a high rate of LR if radiation was delayed in order to first deliver adjuvant chemotherapy, but if negative margins were achieved, there was no adverse affect of radiation delay in local control (55).
TABLE 35-4 Effect of Systemic Therapy on In-Breast Recurrence Rates in Patients Treated with Breast-Conserving Surgery and Radiation Therapy
Study (Reference)
No. of Patients: Selection, Type of Systemic Treatment

 Breast Cancer Screening
Breast Cancer Screening
 Ductal Carcinoma In Situ and Other Intraductal Lesions: Pathology, Immunohistochemistry, and Molecular Alterations
Ductal Carcinoma In Situ and Other Intraductal Lesions: Pathology, Immunohistochemistry, and Molecular Alterations
 Adjuvant Systemic Therapy: Endocrine Therapy
Adjuvant Systemic Therapy: Endocrine Therapy
 Preoperative Endocrine Therapy for Operable Breast Cancer
Preoperative Endocrine Therapy for Operable Breast Cancer



